In a previous blog, I listed 12 reasons to support the view that a high fat diet and an elevated cholesterol or LDL have little to do with heart attacks and another dozen explaining why stress is much more important. So why are we still being told to avoid fat and take statins to lower cholesterol and LDL as much as possible to prevent a heart attack? The answer is very simple: “Follow the money”.
Statins have been the most profitable drugs ever and currently bring in $35 billion/year because they lower LDL “bad” cholesterol”. But there is no such thing as “bad” or “good” cholesterol. LDL and HDL are lipoproteins, not cholesterol. The observation that they are statistically associated with more or less coronary heart disease doesn’t mean they have a causal relationship since there is no proof that raising or lowering them has a predictable effect.
There are well over 300 such statistical associations, including a deep earlobe crease, premature vertex baldness, a potbelly, or living in Glasgow. But having plastic surgery on your ears, a hair transplant, tummy tuck or moving to Honolulu will not reduce your likelihood of having a heart attack. While these are referred to as “risk factors”, which implies causation, “risk marker” would be more accurate.
This confusion between association and causation started in the 1950s, when Dr. Ancel Keys visited Naples, where he found almost no coronary heart disease patients under the age of 60. The only exception was a small class of wealthy people who dined on meat almost daily. In contrast, the general population only had meat once a week or less and mostly ate simple pasta, fruits and vegetables. He also found average cholesterol levels to be low save for the upper class, and assumed this confirmed the causal links between a high fat diet, high serum cholesterol and heart attacks.
Keys subsequently embarked on his famous Seven Countries Study in healthy middle-aged men that showed an amazing straight-line relationship between saturated fat consumption, serum cholesterol and deaths from coronary disease. In East Finland, where serum cholesterol averaged over 260, the number of fatal heart attacks per 1,000 men over a 10-year period was 70. In contrast, Japan had less than 5 such deaths, which Keys attributed to the fact that their average cholesterol was only 160. The contribution of saturated fats to the total daily caloric intake in Finnish men was over 20%, almost ten times higher than the 2.5% for Japanese men. This was widely heralded as definitive proof that risk of fatal heart attacks was proportional to the blood cholesterol level, which, in turn, was proportional to saturated fat intake. Keys was on the cover of the January 13 1961 issue of Time magazine and one leading authority triumphantly proclaimed, “No other variable in the mode of life beside the fat calories in the diet is known which shows such a constant relationship to the mortality rate from coronary or degenerative heart disease”.
The problem is that while Keys had 22 countries to choose from, he “cherry picked” only those that had both high fat intake and high coronary death rates to support his theories. Had he reported the data on all countries he would have come to a very different conclusion. Mexico, which had the same high fat consumption as Finland, was not included because coronary deaths were seven times higher in Finland. Also omitted were Sweden, Germany, France and Israel, where the higher the saturated fat and cholesterol intake, the lower the incidence of coronary deaths.
The World Health Organization’s MONICA (Monitoring of Trends and Determinants in Cardiovascular Disease), a huge epidemiologic study, assessed 21 countries over 10 years. It also failed to find any correlation or connection between heart attacks and fat consumption or cholesterol. As noted below, every single country with the highest fat consumption had the lowest mortality rates from heart disease.
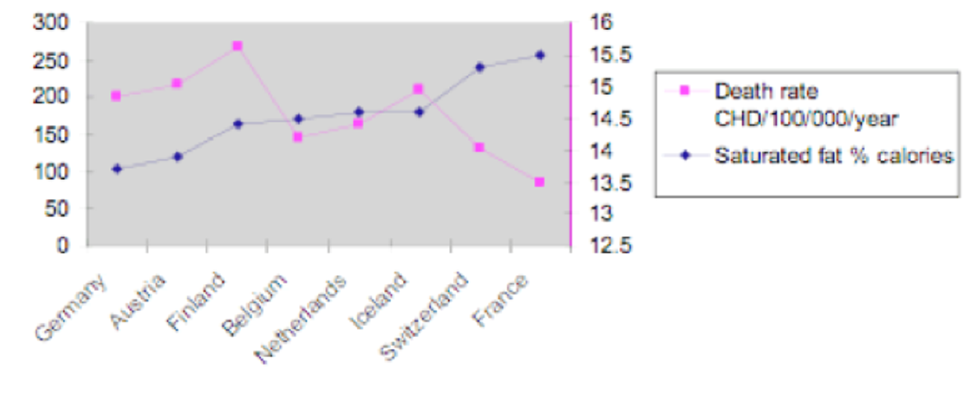
The eight lowest saturated fat consumption countries had the highest CHD death rates, as shown below.
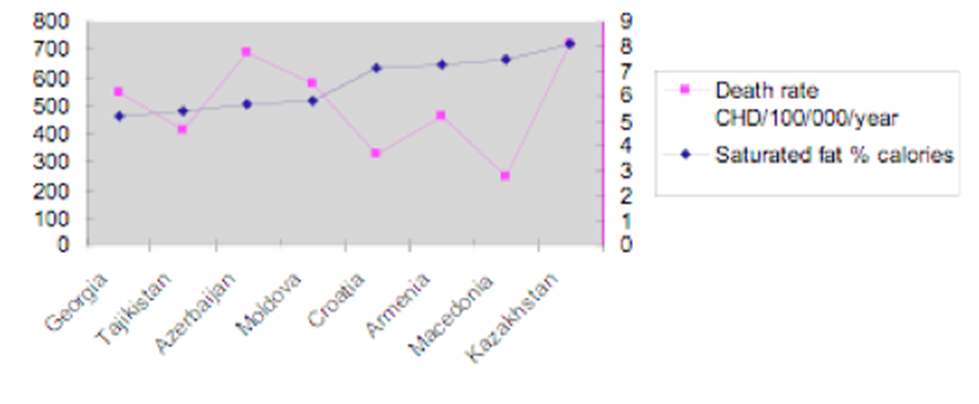
The French consumed three times as much saturated fat compared to Azerbaijan but had one-eighth the rate of heart disease
The NIH had also launched its study of the residents of Framingham, a small manufacturing town in Massachusetts, to confirm Keys theory. It provided the first “solid evidence” that people with a high cholesterol were more likely to have a heart attack and that smoking and hypertension also increased risk. It subsequently showed that these risk factors had additive effects but attempts to prove this were a dismal failure. The huge long-term MRFIT (Multiple Risk Factor Intervention Trial) demonstrated that eliminating all three of these Framingham risk factors did not reduce coronary morbidity or mortality, and a subset of hypertensives treated with diuretics had the highest death rates. In contrast, two other studies conducted during the same period proved so successful they were halted prematurely so that controls would not be denied the benefits of the intervention. One was designed to reduce type-A coronary-prone behavior and the other was treatment with a beta-blocker. The protective effect in both instances was most likely due to lowering the effects of stress-related catecholamine secretion, known to produce cardiac damage and sudden death.
Dr. George Mann, a respected nutritionist and one of the original Framingham investigators, called the diet-cholesterol hypothesis of coronary heart disease “the worst fraud ever perpetrated on the American Public”. Like Kilmer McCully, Uffe Ravnskov and others who also exposed this scam, he was viciously persecuted by the cholesterol cartel. Additional information on all the above can be found at www.stress.org.
Paul J. Rosch, MD, FACP
Dr. Paul J. Rosch is current Chairman of the Board of The American Institute of Stress, Clinical Professor of Medicine and Psychiatry at New York Medical College, Honorary Vice President of the International Stress Management Association and has served as Chair of its U.S. branch. You can follow AIS on Twitter, watch AIS videos on You Tube, become a fan of AIS on Facebook and subscribe to one or both free AIS magazines to receive the latest stress information and research from around the globe directly to your inbox.