SPECIAL ISSUE
The Mammalian Stress Mechanism Explains COVID, Long COVID and Sudden Death
By Lewis S. Coleman, MD, FAIS
*This is an article from the Summer 2023 issue of Combat Stress
COVID vaccines may be deadlier than COVID pneumonia. The “novel” COVID coronavirus disrupts the pulmonary vascular endothelium, which activates harmful pulmonary and systemic mammalian stress mechanism (MSM) hyperactivity that manifests as pneumonia, pericarditis, myocarditis, infertility, loss of hair, taste, and smell, and blood hypercoagulability that invites myocardial infarction, strokes, pulmonary embolus, and congestive heart failure. However, the virus itself remains confined to the lung. The mRNA COVID immunizations introduce the COVID “spike protein” into systemic circulation, where it attacks the vascular endothelium throughout the body. This sometimes mimics contagious COVID, but it also causes covertly increasing blood hypercoagulability that triggers disseminated intravascular coagulation (DIC) without warning, beginning in small peripheral arteries. This disrupts oxygen transport and causes sudden death in some young healthy victims and lingering “Long COVID syndrome” in others. Lingering post-COVID MSM hyperactivity exaggerates the risk and severity of cancer, heart disease, and chronic illness.
Introduction
This special issue of Combat Stress magazine will argue that viral virulence is mediated by the “spike protein,” a single factor, which causes all the confusing and seemingly unrelated pathologies of COVID, its congeners, and its immunizations, by inducing harmful hyperactivity in the newly discovered mammalian stress mechanism (MSM) that disrupts normal physiology. The MSM indicates fresh treatments that reinstate health and save lives by restoring normal physiology.
Viral Virulence
Coronaviruses, like all “common cold” viruses, are obligate intracellular parasites that hijack lung cells to replicate themselves and induce coughing and sneezing that spreads viral particulates to additional victims. Variable viral virulence is not a mutation (an alteration of DNA), but rather an innate characteristic of the viral genome that is lacking in bacteria. Normally the virulence is exaggerated by victim crowding and constrained by viral lethality, but it can be artificially exaggerated.1,2 Exaggerated viral virulence thus explains why the common cold becomes more common during winter, when people are crowded together indoors, and why influenza killed more people than bullets and bombs during WWI after flu-stricken Soldiers were quarantined together in close quarters.3 Variable virulence, however, does not explain the appearance of “novel” coronavirus contagions during peacetime, or why they wax and wane unpredictably at random locations.

Conventional medical theory cannot explain the confusing symptoms and manifestations caused by the virulent “novel” coronavirus, which caused the recent SARS, MERS, COVID-19, and OMICRON contagions. Some have speculated that autoimmune activity causes COVID pathologies, but there is no convincing evidence that immune activity is harmful.4 Others have speculated that a “neurological disease” causes the lingering muscle weakness, fatigue, and “brain fog” of the “Long COVID” syndrome suffered by survivors, but this doesn’t readily explain hypercoagulability, hypertension, heart attacks, strokes, pulmonary emboli, increased cancer, sudden death, stubborn bacterial infestations, unexplained anemia, loss of hair, smell, and taste, or sudden death in healthy young individuals.4-8
There is growing concern that mRNA COVID vaccines cause sudden deaths in young, healthy people by propagating “spike proteins” throughout the body, causing myocarditis and pericarditis that provokes “cytokine storm,” fatal dysrhythmias, and “Commotio cordis”9-41 but this explanation seems weak for several reasons:
- Pericarditis and myocarditis cause warning symptoms of chest pain, fatigue, and malaise before they cause fatal dysrhythmias, but COVID-related sudden death occurs without warning symptoms.42,43
- Myocarditis and pericarditis cause heart failure and hypotension rather than hypertension.26
- Myocarditis and pericarditis resolve slowly, so they are inconsistent with the speedy recovery of victims of unexpected pulseless collapse who were successfully resuscitated by prompt CPR and defibrillation.44-46
- COVID-related sudden deaths resemble catecholamine injury rather than pericarditis and myocarditis at autopsy.47,48
- Pericarditis and myocarditis doesn’t readily explain stroke and pulmonary embolism.26,29
- “Commotio cordis” (fatal spontaneous cardiac dysrhythmia) is a diagnosis of exclusion, when no other explanation is available.
- The inflammation of the vascular endothelium caused by mRNA vaccines is not limited to the heart; it afflicts organs and tissues throughout the body, and the blood hypercoagulability and “Long COVID” symptoms cannot be explained by cardiac effects alone.5,26,30,44,49-55
The “novel” coronavirus that caused human, chicken, and mink epidemics has much in common with the influenza virus that caused the devastating “Spanish Flu” epidemic in 1918:
- Both viruses afflict euthermic mammals and birds.
- Both cause contagions.
- Both afflict the pulmonary endothelium and cause life-threatening “adult respiratory distress syndrome” (ARDS); abnormal bleeding from intestines, eyes, ears, nose, and mouth; sudden death in young, healthy individuals; and lingering muscle weakness, fatigue, loss of hair, smell, taste, and other disabilities in survivors.3,22,23,26,27,33,37,44,49,50,56-78
The WWI influenza deaths were often attributed to secondary bacterial infections, but bacterial effects cannot explain why so many young, healthy people died suddenly without warning symptoms, sometimes within 12 hours of exposure;79 why many bled abnormally; or why survivors suffered lingering muscle weakness, fatigue, and loss of hair, smell, hearing, and taste.
The similarities of COVID and epidemic influenza suggest that the same virulence characteristic caused the mayhem of these otherwise innocuous viruses. I hypothesize that this characteristic is embodied in the “spike protein” that is produced by the coronavirus and found in the tissues of COVID and COVID immunization victims.
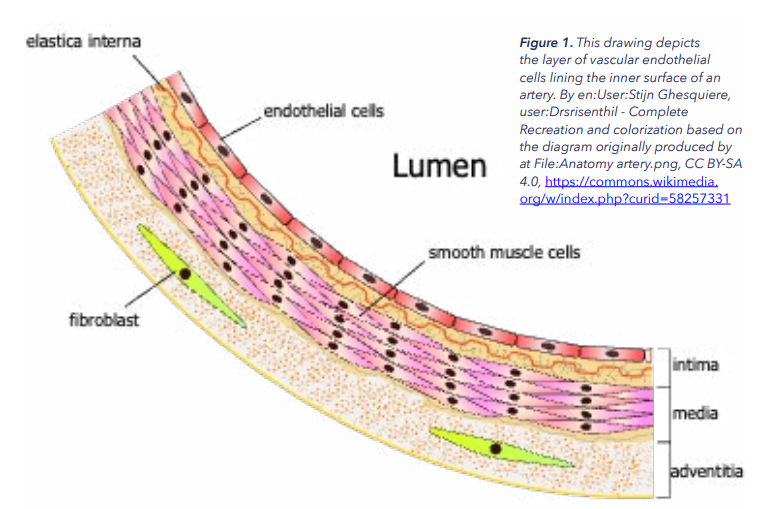
Figure 1. This drawing depicts the layer of vascular endothelial cells lining the inner surface of an artery. By en:User:Stijn Ghesquiere, user:Drsrisenthil – Complete Recreation and colorization based on the diagram originally produced by at File:Anatomy artery.png, CC BY-SA 4.0, https://commons.wikimedia.org/w/index.php?curid=58257331
Stress Theory
Stress theory postulates the presence of a “stress mechanism” that simultaneously regulates tissue repair and organ function, and that hyperactivity of this hypothetical mechanism due to unremitting environmental stresses is the cause of disease. Theoretically, the discovery of such a mechanism would confer fresh treatments directed at its cause and revolutionize medicine.
Theories remain useless until they can be tested and confirmed, and powerful new theories typically arrive many years before evidence becomes available to confirm them.80 For example, Miescher hypothesized that DNA retains and replicates genetic information in the late 1800’s, but his idea remained useless until Watson and Crick discovered and described the DNA structure sixty years later, in 1953.
The DNA discovery inspired an intense international search for the stress mechanism that lasted 30 years and consumed the careers of hundreds of trained researchers, the lives of thousands of tortured test animals, and millions (today billions) of dollars, but it failed to find any clue of the hypothetical stress mechanism, whereupon stress theory was relegated to the realm of the Unicorn and mostly forgotten. Another 30 years of accumulating information from unrelated research finally enabled its discovery by this unlikely amateur.80,81 Thus discovered, the stress mechanism fulfills all the predictions and expectations of the old stress researchers.81 It explains the nature of embryology, physiology, pathology, stress, and their relationships, and it provides a fresh, simplified, cohesive explanation of the confusing effects of COVID and influenza epidemics, as well as mRNA COVID vaccines.
The Mammalian Stress Mechanism (MSM)
The stress mechanism consists of the vascular endothelium, the nervous system, and hepatic “coagulation” enzyme factors VII, VIII, IX, and X. The vascular endothelium is the focus of stress mechanism activity. It is a diaphanous layer of specialized cells, one cell thick, that lines the inner surface of all blood vessels and is the sole constituent of capillaries (see figure 1). It is therefore ubiquitous throughout the body, and it is sub-specialized to suit the requirements of various organs and tissues, which partially explains their differing reactions to stress (see figure 2).
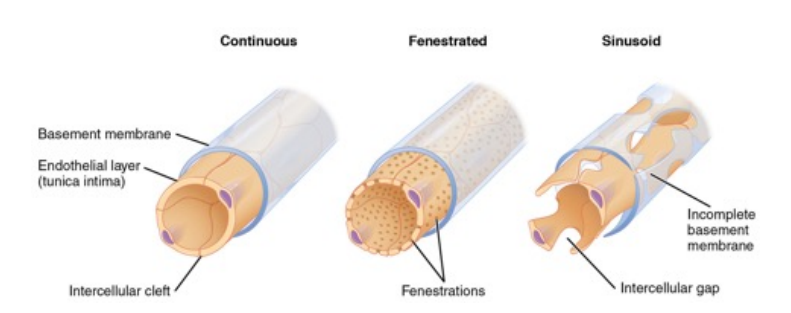
Figure 2. Capillary endothelium is specialized to serve the functions of organs and tissues. It is sinusoid in the liver to facilitate lipoprotein absorption, continuous in the brain to prevent the escape of tissue factor into systemic circulation, and fenestrated in muscle to foster nutrient uptake. By OpenStax College – Anatomy & Physiology, Connexions Web site. http://cnx.org/content/col11496/1.6/, Jun 19, 2013., CC BY 4.0, Link
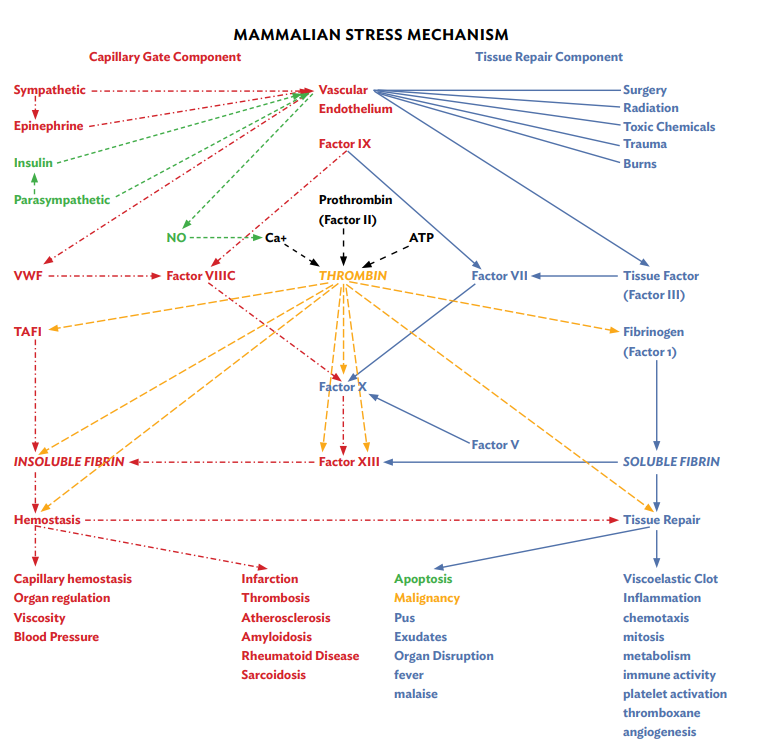
Figure 3. This diagram of the MSM illustrates the relationships of the vascular endothelium with blood enzymes, trauma, and nervous activity. Fluctuating factors VII and VIII alter the enzymatic interaction of factors VII, VIII, IX, and X to determine the location, magnitude, and speed of production of thrombin, soluble fibrin, and insoluble fibrin to repair tissues and regulate organs. Their constant fluctuation focuses MSM effects that repair tissues and regulate organs, but fluctuating hyperactivity of the mechanism produces a bewildering blizzard of symptoms and manifestations that obscures its relatively simple operation.
The vascular endothelium performs several functions:
- It isolates extravascular tissues from flowing blood, so that trauma initiates tissue repair by exposing blood enzymes to tissue factor in extravascular tissues.
- It manufactures von Willebrand Factor (VWF) and releases it into flowing blood in accord with sympathetic nervous activity to “close” the capillary gate mechanism and inhibits organ function.
- It manufactures nitric oxide (NO) and releases it into blood in accord with parasympathetic nervous activity to “open” the capillary gate mechanism and promote organ function.
- It produces several other enzymes and substrates pertinent to stress mechanism operation including ATIII, fibronectin, vitronectin, and protein C.
- Combinations of fluctuating autonomic balance and tissue damage determine how and where the MSM generates its products, which are thrombin, soluble fibrin, and insoluble fibrin.
- Thrombin is the “universal enzyme of extracellular energy.” It enables extracellular cells and enzymes to use ATP energy to enable tissue repair and capillary gate activity. When produced in excess it causes inflammation, fever, malaise, immune activity, cell proliferation and malignancy.
- Soluble fibrin is the “universal substrate of body proteins” including insoluble fibrin, collagen, elastin, lipoproteins, mucus, saliva, and Mother’s milk. When produced in excess it causes edema that disrupts organ function.
- Insoluble fibrin is the “universal polymer of hemostasis.” It enables coagulation, capillary hemostasis, scab formation, and capillary gate operation. When produced in excess it causes hypercoagulability of blood that invites infarction and amyloid production that causes rheumatoid diseases.
The vascular endothelium orchestrates stress mechanism activity via two independently activated sub-components, each of which exaggerates the activity of the other via the enzymatic interaction of factors VII, VIII, IX, and X, which generates thrombin, soluble fibrin, and insoluble fibrin (see figure 3). The constant fluctuation of the sub-mechanisms focuses stress mechanism effects and generates “positive feedback” to repair tissues and regulate organs:
- The tissue repair component repairs tissues in accord with tissue damage. Surgery, sepsis, trauma, burns, radiation, toxic chemicals, viruses, and so forth disrupt the vascular endothelium and expose tissue factor in extravascular tissues to factor VII in flowing blood. This activates factor VII enzyme activity in a dose-related manner, which causes the enzymatic interaction of factors VII, VIII, IX, and X to generate thrombin that energizes tissue repair activities including hemostasis, inflammation, chemotaxis, mitosis, metabolism, immune activity, cell hormone release, cell de-differentiation, cell re-differentiation, and angiogenesis.82
- The Capillary Gate Component governs microvascular flow resistance in accord with autonomic balance, which fluctuates in accord with all forms of nervous activity. Sympathetic nervous activity releases VWF from the vascular endothelium into blood to close the capillary gate, and parasympathetic nervous activity releases nitric oxide (NO) from the vascular endothelium to open it. Carbon dioxide regulates oxygen transport and delivery by directly releasing NO from the vascular endothelium to open the capillary gate.83 Autonomic balance thus regulates organ perfusion, which governs organ activity.84
The stress mechanism repairs tissues and regulates organs efficiently and unobtrusively, but like any mechanism, it has its limits. Excessive and unremitting combinations of nervous stimulation and tissue disruption can induce MSM hyperactivity. This causes the mechanism to waste its substrates and produce harmful excesses and defective versions of its products, which are thrombin, soluble fibrin, and insoluble fibrin. Such stress mechanism hyperactivity manifests as disease.
The lungs are exquisitely vulnerable to viral attack due to their specialized structure and direct exposure to airborne pathogens. Lungs are composed of alveoli, which consists of a single layer of pneumocytes that are surrounded by specialized capillaries that bathe their outer surface in blood. The capillaries consist of a single layer of endothelial cells whose basement membrane fuses with that of the pneumocytes.81,85 This delicate, thin interface optimizes gas exchange in the lung.83
The lungs, brain, retina, nerves, arteries, gonads, placenta, and cervix are rich in tissue factor.86 This amplifies tissue repair mechanism activity, which enhances coagulation and tissue repair, but it also exaggerates the vulnerability of these “target tissues” to stress and cancer.
The vascular endothelium of internal organs, especially in lung, brain, and bowel, is directly innervated by autonomic nerves that regulate the capillary gate mechanism in accord with autonomic balance.81 This exaggerates the sensitivity of these organs to stress.
The lungs and brain are especially vulnerable to stress and malignancy, because they are rich in both tissue factor and autonomic innervation.
Insulin and epinephrine are released into blood in accord with autonomic balance to regulate the capillary gate in peripheral muscles and tissues that are lacking in direct autonomic innervation. Epinephrine releases VWF from the vascular endothelium to close the capillary gate, but brain tissue is protected from ischemia by astrocytes that produce TPA (tissue plasminogen activator). Insulin releases NO from the vascular endothelium to open the capillary gate.
More detailed and fully-referenced explanations of the stress mechanism and its implications, and detailed explanations of blood turbulence and DIC can be found in my published papers,81,84,87-93 which can be downloaded from my website www.stressmechanism.com, or in my book, 50 Years Lost in Medical Advance: The Discovery of Hans Selye’s Stress Mechanism, available via Amazon.com.94
Normal COVID and the Common Cold
The ordinary coronavirus produces “spike protein” that attacks the vascular endothelium and enables the virus to invade its cells, where it hijacks cell machinery to replicate itself. This exposes tissue factor in the lung to factor VII in blood. Tissue factor stabilizes factor VII, which generates thrombin that energizes immune activity, inflammation, and pulmonary exudate (mucus) production. This causes coughing and sneezing, which produces clouds of viral particulates that spread the infection to additional victims until the increased mucus production and immune activity rids the virus from the body.
Inflammation increases the permeability of the pulmonary endothelium, which exaggerates the “leakage” of tissue factor from lung tissues into flowing blood, where it increases factor VII activity. This exaggerates the enzymatic interaction of factors VII, VIII, IX, and X, which amplifies thrombin generation and increases systemic inflammation that exaggerates cellular metabolism throughout the body. This wastefully converts ATP energy into heat. These systemic effects explain the fever, fatigue, and malaise caused by the common cold. However, these symptoms are normally mild and self-limiting, and cause little lasting harm in healthy individuals.
The ”Novel” Coronavirus, COVID, and Critical Illness
Orthodox medicine assumes that individual diseases have independent causes and require individualized treatment regimens, but stress theory explains stress mechanism hyperactivity induced by combinations of environmental stresses is the cause of disease. Thus, all forms of disease are essentially the same, except that the stress mechanism reacts in different ways to different environmental stresses. Thus, treatments that control stress mechanism hyperactivity can restore effective organ function and cure all forms of illnesses.
Critical illness is severe MSM hyperactivity that disrupts organ function and threatens survival. This occurs in a wide variety of stressful circumstances, including major trauma, sepsis (systemic bacterial infestation), pneumonia, extensive invasive surgery, poison exposure, major burns, pregnancy, cardiac bypass, and so forth. Conventional medical theory cannot explain critical illness, and can only describe “syndromes” (groups of symptoms that collectively indicate or characterize a disease). For example, critical illness that occurs during pregnancy is called “eclampsia.” The “Surgical Stress Syndrome” (SSS) occurs when general anesthesia is inadequately supplemented with analgesia during surgery. “Systemic Inflammatory Response Syndrome” (SIRS) occurs when anesthetized patients subjected to coronary artery bypass are inadequately supplemented with narcotic analgesia. However, these syndromes are often confused with one another because their symptoms are similar. They are all essentially the same phenomenon, because all of them are caused by severe stress mechanism hyperactivity.
The “novel” coronavirus is more virulent than the normal coronavirus, so that it causes considerably greater stress mechanism hyperactivity that manifests as inflammation, immune activity, and exudate production. This manifests as “viral pneumonia” or “adult respiratory distress syndrome” (ARDS), which is a life threatening “critical illness” because it produces excessive pulmonary exudates that disrupt gas exchange, promote pulmonary sclerosis, and release excessive quantities of tissue factor from the lung into systemic circulation, causing systemic inflammation that disrupts organ function.
Patients who suffer from pre-existing chronic illnesses (“rheumatoid” diseases) and obesity are vulnerable to develop “critical illness” when they are afflicted by the novel coronavirus. This is because chronic illness causes tissue sclerosis and accelerates capillary senescence that compromises oxygen transport and delivery, and undermines organ function.83 These harmful effects exaggerate the morbidity and mortality of MSM hyperactivity induced by the “novel” coronavirus.
The effects of COVID pneumonia are not limited to the lung, because it causes harmful systemic effects. The lung is rich in both tissue factor and autonomic innervation. COVID pneumonia releases tissue factor from the lung into systemic circulation, where it activates blood enzyme factor VII. It simultaneously exaggerates harmful sympathetic nervous activity that releases von Willebrand Factor (VWF) from the vascular endothelium into flowing blood. VWF activates factor VIII, which increases the conversion of fibrinogen into soluble fibrin and insoluble fibrin. The soluble fibrin penetrates through the inflamed vascular endothelium into inflamed organs and tissues, where it causes tissue edema that disrupts organ function. The insoluble fibrin exaggerates blood viscosity (flow resistance) and coagulability, which invites embolism and infarction that threatens oxygen transport and delivery. These harmful effects disrupt the function of one organ after another. This progressive organ disruption is called “Multi-Organ Failure Syndrome” (MOFS).
The brain is the next organ to be afflicted, because like the lung it is rich in tissue factor and autonomic innervation. Brain inflammation manifests as delirium and dementia that culminates in coma, and it releases still more tissue factor into systemic circulation.
The increasing MSM hyperactivity disrupts the glycocalyx, which is a delicate molecular mesh produced by the vascular endothelium that lines the interior surface of all blood vessels.95-97 This releases albumen protein from the glycocalyx into flowing blood, and it accumulates in renal tubules along with soluble fibrin (“hyalin”) to form “casts” that clog the renal tubules and halt urine production. This is called “Acute Renal Failure” (ARF). If the condition persists, it causes permanent kidney damage that is called “Chronic Renal Failure” (CRF).95,97-99 The soluble fibrin appears in urine and is called “proteinuria.” The albumen appears in urine and is called “albuminuria.” These detectable changes warn of increasing MSM hyperactivity.
As soluble fibrin invades tissues, it causes visible edema of the skin. It also invades organs and disrupts their function. This sometimes causes the liver to swell and burst.100 It also invades bowel tissue, which halts peristalsis. This is called “bowel ileus.”
Meanwhile, rising blood levels of insoluble fibrin exaggerate blood viscosity (microvascular flow resistance) and coagulability. This inhibits the ability of the turbulent pulse waves to maintain arterial patency by preventing clot formation. Rising blood coagulability invites myocardial infarction, stroke, and pulmonary embolus. If blood coagulability rises above a critical threshold, then spontaneous “disseminated intravascular coagulation” (DIC) may unexpectedly occur. In the context of critical illness, this manifests as unexplained bleeding from eyes, nose, mouth, ears, and subcutaneous tissues, and often culminates in death.
Disseminated Intravascular Coagulation (DIC)
Disseminated Intravascular Coagulation (DIC) is sudden, spontaneous arterial coagulation combined with unexplained bleeding. It is clinically confusing, because coagulation involves a fluctuating balance of factors that promote and prevent coagulation, and many of these factors remain unappreciated. Perhaps the most important such factor is pulsatile blood turbulence, which maintains arterial patency by inhibiting atherosclerosis and clot formation, and disintegrating intra-arterial clots that obstruct arterial flow.87,88,91,93
Red cell mass affects arterial blood turbulence. The small size, biconcave shape, and neutral buoyancy of mammalian red blood cells causes them to spontaneously form “Rouleau” or “stacks” that inhibit turbulent flow resistance. This enhances mammalian exercise tolerance, but if red cell mass becomes excessive, it can inhibit arterial turbulence to the point that DIC begins spontaneously. For example, overenthusiastic treatment with Epogen, which is artificial erythropoietin that is used to treat anemia, can dangerously elevate red cell mass and cause lethal DIC.7,101 Another example is “blood doping” by athletes who dose themselves (illegally) with Epogen in order to optimize their exercise tolerance and athletic performance.102 This is a dangerous practice and has caused DIC deaths.103 On the other hand, severe anemia, such as occurs during severe chronic renal failure, can exaggerate pulsatile blood turbulence to the point that hemostasis fails, and uncontrolled bleeding occurs.104,105 The exaggerated turbulence also increases blood viscosity (flow resistance), which undermines oxygen transport and delivery to tissues, and causes oxygen starvation. This explains why severe anemia causes chronic fatigue, weakness, and poor exercise tolerance.105,106 This can be treated with transfusions of packed red blood cells that reduce turbulence and restore effective coagulation.
Yet another factor that affects blood coagulation is MSM hyperactivity that elevates insoluble fibrin generation in blood. Insoluble fibrin exaggerates blood coagulability, inhibits pulsatile turbulence, and binds red cells together into clots.88 Rising levels of insoluble fibrin inhibit pulsatile turbulent flow resistance and enhance cardiac efficiency until it lowers pulsatile turbulence below a critical threshold, whereupon spontaneous DIC begins.
DIC begins in small peripheral arteries, where turbulence declines exponentially with increasing coagulability. If it proceeds rapidly, it can disrupt oxygen transport and delivery, causing sudden death. More often, it consumes, wastes, and depletes coagulation substrates including fibrinogen, fibronectin, and vitronectin, and forms defective clots that remove red cells from circulation and deposits them on the inner walls of arteries. The resulting anemia exaggerates turbulence, which increases flow resistance and inhibits coagulation.105,106
This provides a brief introduction to DIC details pertinent to this presentation. Those who seek a more thorough and fully referenced explanation of this confusing subject can find it in my book.94
COVID Immunizations, Sudden Death, and Long COVID Syndrome
The COVID mRNA vaccines may be more dangerous than COVID itself,49,107-109 because vaccine introduces viral elements directly into systemic circulation, where they cause cells to propagate harmful “spike protein” throughout the body. This causes the vascular endothelium to release VWF into systemic circulation, which activates factor VIII that generates insoluble fibrin. This inexorably elevates blood coagulability, which invites infarction, embolus formation, and DIC.
In older patients, whose microvascular perfusion is compromised by capillary senescence, the rising blood coagulability elevates the risk of myocardial infarction, stroke, and thrombosis.109 The DIC produces microthrombi that clog capillaries, and forms abnormal calamari-like strands of insoluble fibrin that occlude small peripheral arteries, halt cardiac function, disrupt oxygen transport and delivery, and persist after death.68 However, the calamari strands are typically discovered during embalming rather than autopsy, because conventional autopsy focuses on large central arteries and coronary arteries rather than small peripheral arteries.
Healthy young people develop a more vigorous stress response to COVID and influenza epidemics than elderly victims, which explains why the victims of sudden death are predominantly young and healthy.24,41,109,110 In younger patients, whose microvascular circulation remains intact, the increasing blood coagulability doesn’t cause warning symptoms until it rises above a critical threshold, whereupon it triggers disseminated intravascular coagulation (DIC) that suddenly and unexpectedly disrupts oxygen transport and delivery. This causes brain hypoxia, loss of consciousness, and sudden death. The deaths are painless, because the brain cannot detect pain in its own tissues, and it quickly depletes its supply of oxygen, which extinguishes consciousness before painful hypoxia develops in other organs and tissues. This occurs so quickly that the calamari strands do not develop, and plasmin activation disintegrates the causative clots soon after death, leaving only the inflamed vascular endothelium as evidence. As a result, most DIC deaths in healthy young people are attributed to myocarditis, pericarditis, cardiac tamponade, or congestive heart failure, even though these conditions typically cause warning signs of fatigue and malaise before causing death.111 Instead, the autopsies report that the heart is distended, as if the patients died of catecholamine overdose, but this cannot be explained by conventional theory.47,51,112 This cardiac distention is explained by the sudden obstruction of cardiac ejection due to DIC. 17,20,32,42,44,51,64,65,67,68,78,113-117 The phenomenon is fleeting, because some victims are successfully resuscitated when trained CPR technicians and defibrillation equipment are immediately available. Such survivors sometimes exhibit abnormal unexplained bleeding in lungs and body orifices.44,45,116,117 This is consistent with spontaneous clot disintegration due to plasmin activation.
DIC is not invariably lethal. Sometimes the DIC process removes red cells from circulation, causing anemia which exaggerates pulsatile turbulence that halts the clotting process before it becomes fatal. However, the abnormal coagulation clogs small arteries and capillaries, and causes anemia that exaggerates turbulent flow resistance, as in patients with the anemia of chronic renal failure. The increased flow resistance inhibits oxygen transport and delivery, which manifests as fatigue, muscle weakness, and mental “fog.” The small renal arteries are especially vulnerable to clogging by the abnormal coagulation, which explains why many patients suffer intense hypoxic renal pain after COVID injections. The abnormal coagulation may also cause lasting damage to the arterial tree and capillaries that undermines oxygen transport and delivery, which explains persisting muscle weakness, fatigue, mental “fog” and vulnerability to stubborn infections. It also increases flow resistance, which exaggerates cardiac work and promotes congestive heart failure.118,119
Meanwhile, as the spike protein attacks the vascular endothelium throughout the body, it causes pericarditis, myocarditis, pericardial effusions, cardiac tamponade, miscarriages, testicular edema, infertility, malaise, lingering loss of hair, smell, and taste, and stubborn infections.18,30,39,42,115,120,121 Furthermore, the lingering MSM hyperactivity exaggerates the risk and severity of cancer, heart disease, and chronic illnesses.30,56-60,70,74,113,121,122 In some patients these symptoms and conditions persist for months or even years, and they account for the “Long COVID syndrome” that occurs after mRNA immunizations.41
Pre-existing Illness and COVID
Pre-existing chronic illnesses exaggerate the severity of COVID and influenza contagions. Chronic illnesses have been increasing exponentially for years on account of environmental pollution.123 They include seemingly unrelated conditions including diabetes (type I and type II), hypertension, atherosclerosis, systemic lupus erythematosus (SLE), Sjogren’s Disease, scleroderma, Parkinson’s Disease, Alzheimer’s disease, polymyalgia rheumatica, rheumatoid arthritis, gout, and multiple sclerosis. Conventional medicine classifies these illnesses as “rheumatoid diseases” or “autoimmune” diseases. However, there is no convincing evidence that immune activity per se causes them.
Many chronic illnesses are closely associated with specific forms of environmental stress. For example, obesity is closely associated with atherosclerosis, hypertension, and diabetes; SLE is associated with cosmetics exposure; and Parkinson’s disease is closely associated with pesticide exposure. Conventional medical theory cannot explain these observations.
The nature of chronic illnesses supposedly remains unknown, but the research literature reveals that rheumatoid diseases invariably involve amyloid protein accumulation in their afflicted tissues. Conventional medicine ignores this and views amyloidosis as a rare, mysterious, and unrelated disease. The MSM explains amyloidosis. Unrelenting environmental stresses such as pesticides, herbicides, automobile exhaust, chlorinated water, and industrial pollution increasingly contaminate the beverages we drink, the food we eat, and the air we breathe. To this may be added the emotional adversity of difficult marriages, frustrating jobs, and the eternal injustice of government justice, all of which induce stressful nervous activity that harmfully stimulates the MSM. These stresses persistently exaggerate capillary gate activity, which increases the generation of insoluble fibrin and its subsequent disintegration into “fibrin split products” (FSP).124 The FSP is normally harmless and is re-cycled by the body. However, some of the FSP re-interacts with coagulation factor X to produce abnormal “amyloid” protein that accumulates in organs and tissues. Thus, environmental stress exaggerates insoluble fibrin “turnover” and amyloid production. As a result, atherosclerosis and amyloidosis occur in concert, and substantial amyloid accumulation appears in the abnormal clots and strands of insoluble fibrin caused by DIC.125 The amyloid induces subclinical inflammation and immune activity in the afflicted tissues of rheumatoid diseases. It accelerates capillary senescence, which undermines tissue oxygenation that promotes pathological collagen generation that causes debilitating sclerosis in organs and tissues.126-129 Such pre-existing organ and tissue damage exaggerates morbidity and mortality in COVID victims.
Clinical Examples
Though critical details are usually lacking, the following examples gleaned from public reports illustrate how COVID immunizations cause heart attacks, strokes, blood clots, DIC, unexplained sudden death, and Long COVID syndrome.
Example # 1: Susan D.
Although I am a board-certified anesthesiologist with more than 40 years of experience, I failed to notice the controversial deaths and “Long COVID” problems associated with the immunizations until my chance acquaintance with Susan D., a previously healthy 75-year-old school psychologist who was obliged to undergo five Moderna COVID-19 immunizations over a period of 18 months on penalty of losing her job.
Susan’s first four immunizations caused no distress, but her fifth immunization on 9/15/2022 was a “bi-valent booster” which caused sharp pain during the injection. About three minutes later this was followed by weakness, fatigue, fatigue, mental fog, malaise, nausea, chills, and dizziness. The sudden onset of weakness, mental fog, and fatigue is best explained by sudden MSM hyperactivity that triggered a non-lethal episode of DIC that impaired oxygen transport and delivery. Despite these severe symptoms, she drove herself a short distance home, and went to bed. On the following day, 9/16/22, she experienced flu-like symptoms including nausea, weakness, chills, and fatigue. That night she suffered sudden, searing pain in her right flank that was exaggerated by touch (allodynia). The most likely explanation was an abnormal DIC coagulation that obstructed blood flow to her right kidney and caused hypoxic kidney pain. The next morning, 9/17/22, she visited an emergency room, where she was treated with Toradol 30 mg IM to control the pain. A complete blood count (CBC) revealed that her hemoglobin level was 6.5 gm/dL. (half normal). Because of this, she was transfused with a unit of blood and iron pills were prescribed even though a rectal examination revealed no blood and she had no history of black tarry stools or other evidence of blood loss. The most likely cause of this sudden, unexplained onset of severe anemia is DIC that sharply reduced circulating red cell mass. A kidney stone was suspected, and she underwent a CAT scan of her entire body, but the results were negative. That night, 9/18/22, the flank pain resumed, and she returned to the emergency room, where she was treated with another 30mg Toradol IM. This controlled the pain and it never returned. The simplest explanation is that the anticoagulant effects of the Toradol together with increased pulsatile turbulence of anemia disintegrated the blood clot that obstructed perfusion in her right renal artery. A repeat CBC on that occasion showed that the transfusion had raised her hemoglobin to 7.9 gm/dL, which was still low. She continued to suffer fatigue, weakness, exercise intolerance, and mental fog. This reflects the generalized tissue hypoxia she suffered due to her near-lethal episode of DIC that compromised oxygen transport and delivery.
On 10/10/22 she underwent fiberoptic examination of her upper and lower GI tract, which failed to find any evidence of GI bleeding. This confirms my hypothesis that her anemia was caused by DIC. Her doctors, as well as I, were baffled by her lack of trauma, surgery, hematuria, tarry stools, bright red blood in her stools, or any other explanation of her anemia. On 11/27/22, approximately two months after the problematic COVID immunization, she suffered fresh symptoms of COVID, including worsened fatigue, sore throat, a dry cough, and atelectasis. COVID was confirmed by testing on 11/30/22. This is consistent with reports that the COVID immunizations actually cause COVID. By that time her hemoglobin level had risen to 10 gm/dL. This suggests that the abnormal DIC clots had spontaneously disintegrated due to plasmin generation, and the red cells had been re-mobilized by pulsatile blood turbulence that normally maintains arterial patency.130 A subsequent COVID test on 12/11/22 was negative, but as of 12/17/22 she continued to complain of sore throat, shallow cough, headache, atelectasis, fatigue, poor exercise tolerance, and brain fog. Similar symptoms are widely-reported characteristics of the “Long COVID” syndrome.56,57,73,74,131-133
Susan’s symptoms slowly improved, and by Tuesday, 1/10/23 her hemoglobin had reached 11.8 gm/dL, which is essentially normal, and she had returned to using her treadmill machine, and no longer complained of “brain fog.” On 1/12/23 she underwent repeat endoscopy to remove a colon polyp discovered by the previous endoscopy, but this second endoscopy also failed to reveal any source of gastrointestinal bleeding.
I remained as puzzled by Susan’s fatigue and unexplained anemia as her doctors until I discovered a YouTube interview with Dr. Jaco Laubscher, a South African internist who observed that “Long COVID” patients, like DIC victims, exhibit damaged vascular endothelium, increased peripheral blood flow resistance, and hypercoagulable blood, and that anticoagulants relieve their symptoms.”50,58 With this fresh information, plus my understanding of stress theory, I surmised that Susan had suffered an episode of DIC, which explained her unexpected anemia and symptoms of fatigue, muscle weakness, renal pain, and mental fog. Since then, accumulating reports have corroborated my suspicions.31,32,58,113
What is unusual about Susan’s experience is that her CBC test was drawn at a critical moment that revealed the severity of her unexplained anemia. This clue is lacking in most reports. Furthermore, she didn’t exhibit the abnormal bleeding, edema, and skin lesions that typify DIC.
The cause of Susan’s injection site pain and immediate malaise remains unclear, but it invites the following possibilities:
- Her previous COVID immunizations may have exaggerated sensitivity to the vaccine that caused the fifth immunization to be painful.
- The needle might have struck a nerve or periosteum (the innervated sheath surrounding bone).
- The vaccine may have been accidentally injected into a vein, so that it was quickly distributed systemically.
Susan’s sudden symptoms of weakness, fatigue, dizziness, mental fog, nausea, and half normal CBC test immediately following her 5th COVID booster are best explained by DIC that trapped half of her circulating red cell mass in defective clots that were deposited on the inner walls of her arteries. Like the anemia of chronic renal failure, the DIC reduced the circulating mass of red cells, which exaggerated turbulent flow resistance, undermined oxygen transport and delivery, and caused her sudden symptoms of fatigue, weakness, dizziness, nausea, and brain fog. Her right flank pain was most simply explained by abnormal clot formation that obstructed her right renal artery.53 Fortunately, the clot was soon cleared by pulsatile turbulence, which restored perfusion and oxygenation to the kidney, and eliminated the hypoxic kidney pain. As of 1/24/2023 there was no evidence of residual renal damage, and her CBC tests were normal. She still suffers from residual loss of smell, taste, and hair, but has mostly recovered her muscle strength and mental clarity, and she has resumed her normal activities including daily exercise on her treadmill. In my opinion, she is fortunate to have survived without more serious sequelae.
I recommended that Susan obtain a thromboelastography (TEG) or d-Dimer test to assess her blood coagulability and residual risk for continuing MSM hyperactivity, but the “gatekeeper” (family physician) of her medical plan categorically refused consent.
Example #2 Charlbi Dean 65,66
Charlbi Dean was a healthy 32 year old actress who awoke from sleep with the perception of medical distress during the night and alerted her fiancé to take her to the hospital, where she died in his company. She did not complain of pain. I hypothesize that she was awakened by a poorly understood protective brain mechanism that detects hypoxia during sleep and restores consciousness during “obstructive sleep apnea” where the afflicted person repeatedly becomes hypoxic and regains partial consciousness on account of airway obstruction that re-occurs with the return of sleep. Unfortunately, the restoration of consciousness didn’t disrupt the DIC that killed her soon afterwards.
The New York Medical Examiner attributed her death to her previous history of splenectomy that supposedly caused an obscure form of bacterial sepsis, even though her autopsy revealed evidence of a viral infection in her lungs that may have been COVID or an effect of COVID immunization. This is a weak explanation given the absence of any evidence of illness before her sudden death.
Her immunization history was not made public, but her sudden death is most simply explained by DIC secondary to COVID immunization, even though persons suspicious of her cause of death were disparaged as “anti-vaxxers.”65,66 Unfortunately, no blood test results, if any, were revealed to the public, but the limited evidence available suggests that the DIC phenomenon doesn’t necessarily cause immediate death, and that she could have been saved by timely treatment with anticoagulant therapy if her critical condition had been understood.

Example #3 Hunter Brown
Hunter Brown was a healthy 21-year-old cadet at the American Air Force Academy and a valued member of the academy football team. He was undoubtedly immunized for COVID because this is a military requirement.67 He collapsed while walking to class, but there was no ambulance or defibrillation equipment available and CPR failed to save him.
Example #4 As Reported by Debbie Kulick 45
A healthy young woman was walking to a football game with her husband, a trained paramedic, when she suddenly complained that she didn’t feel well, and then collapsed in cardiac arrest to the blacktop in a parking lot. Her husband noted that she did not have a pulse, and immediately called for help and began CPR. Athletic trainers, a doctor, and an ambulance with defibrillation equipment were immediately available. She regained consciousness and resumed breathing after she was defibrillated using an AED and was transported to a hospital. The simplest explanation is that DIC occurred secondary to COVID immunization, soon followed by spontaneous plasmin disintegration of abnormal DIC blood clots that enabled successful CPR and defibrillation that restored oxygen transport and delivery.83 Unfortunately, no revealing blood tests, if any, were made available to the public. As in the case of Charlbi Dean, she remained conscious long enough to realize that she was dying but did not complain of pain. This is consistent with the present understanding that brain viability lingers for several minutes despite oxygen starvation.
Example #5 Autopsies of Two Adolescents Who Died After COVID Vaccination 47
AUTOPSY RESULTS -: The microscopic examination revealed features resembling a catecholamine-induced injury, not typical myocarditis pathology. CONCLUSIONS -: The myocardial injury seen in these postvaccine hearts is different from typical myocarditis and has an appearance most closely resembling a catecholamine-mediated stress (toxic) cardiomyopathy. Understanding that these instances are different from typical myocarditis and that cytokine storm has a known feedback loop with catecholamines may help guide screening and therapy.
These autopsy results are consistent with the hypothesis that DIC suddenly exaggerates arterial flow resistance in the manner of catecholamine injury, halts cardiac function, distends the heart, and disrupts oxygen transport and delivery. This would explain the cardiac enlargement and cardiomyopathy observed at autopsy.
Example #6 Caddie Collapses, Given CPR During AT&T Pebble Beach Pro-Am Golf Tournament 117
“From my perspective, it seemed like we lost him,” Nelson said. “Luckily there was a police officer on the sidelines there and he [performed] CPR. So, he came in and effectively saved his life.”
Higgs said he was then informed the caddie’s condition had improved and that he would be OK.
This incident is interesting because the victim survived without the need for defibrillation, which suggests that spontaneous plasmin disintegration of the defective clots must have enabled successful CPR resuscitation.
Example #7 Yasmin Vossoughian opens up about health scare 42
Yasmin is a news anchor on national television. Her illness illustrates how viral pericarditis, pericardial tamponade, and myocarditis cause chest pain, dyspnea, fever, fatigue, and other warning symptoms. Her cardiologist arbitrarily attributed the illness to “autoimmune activity” but immune activity has never been demonstrated to cause disease. Her pericarditis, which caused the cardiac tamponade, was most likely caused by COVID vaccination. Unfortunately, her vaccination history was not revealed.
Example #8 Princess of Thailand Collapsed after COVID jab 114,134
The healthy 40-year-old daughter of the king of Thailand collapsed suddenly 23 days after her third COVID immunization and remains in a coma. A world-famous expert claims that the COVID immunization caused her collapse. The king is reportedly furious.
Example #9 Elon Musk felt like he ‘was dying’ after 2nd COVID booster shot, and his cousin in ‘peak health’ suffered myocarditis 28
Like Susan, Elon Musk experienced injection site pain, COVID symptoms, and a severe reaction that lasted several days after multiple COVID immunizations and boosters required by his work. He also stated that his cousin, who was in excellent health, suffered cardiac myositis that required hospitalization after he was immunized. He has not provided further details. Most such sudden episodes of medical distress seem to occur within a month of COVID immunization.
Airline Pilots
Both military and commercial airline pilots have always been subject to strict medical standards. It is thus highly unusual for any active pilot to suffer an unexpected medical emergency. However, soon after COVID vaccination became mandatory, pilot Bob Snow suffered a heart attack six minutes after landing his airplane carrying 200 passengers.135 The incident was not investigated by either the airline or the FAA, but soon afterward the FAA loosened EKG standards for pilots, which suggests that cardiac problems have increased since COVID immunizations became mandatory.54,55,136 Perhaps even more disturbing is reports that “co-pilots” may no longer be present on some flights, which implies that airline pilots are now in short supply.137
Here are reports of airline incidents from the month of March 2023:
Example #1
On March 3, 2023 Virgin Australia flight from Adelaide to Perth forced to make emergency landing as First Officer suffered heart attack 30 minutes after departure.138
Example #2
On March 11, 2023 BA TRAGEDY Veteran British Airways pilot collapses and dies shortly before he was due to captain packed passenger jet.139
Example #3
On March 11, 2023, A United Airlines flight from Guatemala to Chicago was diverted to Houston’s George Bush International Airport on Saturday evening. An emergency was declared “for an incapacitated pilot,” stated a Houston UAL internal document given to CDM Press. “UA Flight 2007 GUA-ORD is diverting to IAH. Declaring an emergency for an incapacitated pilot. Gated at E20. Current ETA shows 1747. Unknown if flight will clear here at this time or just re-crew and go. Will advise when information is available. Pilot reportedly taken to a hospital,” states the UAL Operation Center communication. According to the UAL file, “Left seat Capt had chest pains. Could not get him out of the seat. Right seater landed.” On Saturday evening, KHOU-TV Houston reported that the airport spokesperson told that news organization that the flight was diverted “due to a technical issue.” UAL’s CEO Scott Kirby has prided himself for making mandatory covid vaccinations part of UAL’s branding since August 2021 when he first mandated the shots.
At that time, UAL employees could apply for a religious or medical exemption. Kirby has claimed publicly that 99% of their employees have been vaccinated. But, there is more to Kirby’s proclamations. If a religious exemption was granted, employees were put on “unpaid leave.” They did not have access to any of their benefits, including medical, vision, life, and their 401(K) accounts. If they wanted to continue with their medical insurance, they had to make payments which was burdensome because they were not receiving paychecks. It was only in March 2022 when those put on unpaid leave were invited back to work.140
Example #4
On March 13, 2023, Emirates Flight EK205 MXP-JFK from Milan diverted on March.13, 2023 due to pilot illness, returned to Milan for emergency landing – now 4th pilot incident this month. Dubai: Emirates cancels flight, returns to origin destination after take-off.140
Example #5
On Mrch 18, 2023, an Air Transat Airbus A321 was flying from Fort-de-France to Montreal when the aircraft’s first officer became incapacitated. The incident occurred as the aircraft was flying over the United States, 200NM south of Montreal. According to The Aviation Herald, the incident took place aboard Air Transat flight TS739, an Airbus A321-200 service from Fort-de-France, capital of the French territory of Martinique to Montreal, Canada. The flight departed took off at 13:34, 34 minutes past its scheduled departure time. According to FlightRadar24.com data, reached a cruising altitude of FL320 approximately 25 minutes after takeoff. The aircraft increased its cruising altitude twice more during the flight, going up to FL340, and then FL360. 191 people were onboard the A321-200, which was registered C-GTCY.141
Despite two such instances taking place within a week, these cases are thankfully quite rare. However, the top priority for aviation is safety. Thus, the reality of the occasional “incapacitated pilot” incident is one strong argument against the possibility of single pilot operations. Two pilots in the cockpit provide redundancy so that if one of the aircraft’s pilots were to become incapacitated, the other pilot could take over the full operation of the aircraft and perform a landing.
Last month, a Reuters report noted that the European Union Aviation Safety Agency (EASA) had ruled out single-pilot flights by 2030. However, the regulator was reportedly still evaluating proposals from Airbus and Dassault Aviation. This could see limited single-pilot operation for parts of the flight as early as 2027.
It would appear, however, that some proposals for single-pilot operations would still include at least one other pilot onboard the aircraft. This is the case for Airbus and Cathay Pacific’s ‘Project Connect’, which envisions a fatigued pilot being able to rest in the crew rest area while the other pilot flies solo during less-demanding portions of the flight, and not takeoff or landing.141
Example #6 Southwest Boeing 737
On March 22, 2023, a Southwest Airlines flight from Las Vegas (Nevada) to Columbus (Ohio), saw its captain become incapacitated. The Aviation Herald notes that the Boeing 737-700 was en route at FL370 about 160nm northeast of Las Vegas when the first officer radioed air traffic control to notify them that the captain was complaining about stomach pain. It was then noted that the captain then became incapacitated. In a similar resolution to the Air Transat situation, another pilot was available to step in. In this case, it was a passenger that was an off-duty, fully-licensed pilot for a different airline.141
Example #7
On March 28, 2023 TAROM Flight RO-7673 TSR-HRG service from Timisoara (Romania) to Hurghada (Egypt) diverted: 30 year old pilot had chest pain and collapsed in-flight on March 25th, 2023 – 7th pilot incident this month.142
NFL Football Players
95% of all NFL football players are known to be COVID vaccinated as a requirement of their jobs, and a surprising number of these healthy young men have died suddenly without explanation or suffered coagulation abnormalities, strokes, and heart attacks since the appearance of COVID and its immunizations. Blood doping doesn’t explain these problems, because that practice became commonplace among professional athletes long before COVID, and its dangers are well known.7,103 Medical information that might clarify what happened in these cases, such as tests of blood coagulability, CBC results and so forth, are not made available to the public, but unexplained deaths, blood clots, heart attacks, and strokes in healthy young men at any age, especially professional athletes, are rare and noteworthy. The increase in such problems in NFL players since the onset of the COVID contagion is best explained by hypercoagulability of blood secondary to COVID immunizations.

Example #1
Damar Hamlin 44-46,116 was 24 years old when he suddenly collapsed during a nationally televised football game, and he would surely have died were it not for the prompt medical attention he received. He was defibrillated twice on the scene, and then intubated and transported to a nearby hospital, where he was placed in intensive care. Abnormal bleeding from his lungs was reported, but he regained consciousness the next morning and was extubated and sent home a few days later. It remains to be seen whether he will resume his football career. His collapse was attributed to “commotio cordis” but this is a diagnosis of exclusion because no other explanation was available.44 DIC due to COVID immunization is the simplest explanation of his cardiac arrest, abnormal lung bleeding, and swift recovery.
Example #2
Uche Nwareri, a “die-hard vax zealot,” died suddenly at age 38 in his wife’s home.64 His death was attributed to “enlarged heart with acute heart failure.” This diagnosis makes no sense, because Mr. Nwareri had no history of heart failure. The simplest explanation is that abnormal DIC clot formation in small peripheral arteries sharply increased flow resistance, so that his heart became distended because it was unable to empty its contents while he was dying.47
Example #3
Franco Harris was in good health at age 72 until he died suddenly after two COVID injections. His death was dismissively attributed to “natural causes” but COVID immunization is a better explanation.143
Example #4
Jaylon Ferguson died suddenly at age 26. His death was attributed to fentanyl and cocaine abuse, but his known behavior as a loving father and reliable football teammate was inconsistent with drug abuse.144
Example #5
Riddick Parker, Jr. collapsed and died suddenly while riding a bike at age 49.145
Example #6
Alaric Jackson, age 25, had his 2022 season cut short due to blood clots.146
Example #7
Max Mitchell, age 23, also had his 2022 season cut short due to blood clots.147

Example #8
Henry Anderson, age 31 had a stroke and missed several games in 2022.148
Example #9
Jesse Lemonier, age 25, died suddenly January 26, 2023149
Treatment for COVID pneumonia and other forms of Critical Illness
Stress theory suggests the following means for managing life-threatening COVID pneumonia as well as other life-threatening critical illnesses:
- Prevention is preferable to cure. Vitamin D minimizes the risk and severity of COVID and other viral illnesses.73,150-154
- Draconian quarantine measures such as those imposed in China may dangerously exaggerate viral virulence. Such misguided crowding and confinement caused the influenza epidemic that devastated the Athenians in their war with Sparta,155 and the devastating “Spanish Flu” epidemic of WWI.3
- Elective endotracheal intubation protects health care workers from the contagion, provides respiratory support as needed, and enables the measurement of inhaled gas mixtures.
- Generous opioid treatment with modern synthetic opioids such as fentanyl, Sufentanil, or Dilaudid controls the nociception pathway, prevents spontaneous hyperventilation, and promotes beneficial CO2 accumulation.
- Maintain exhaled CO2 concentrations in the range of 50-100 torr to preserve respiratory drive, minimize microvascular flow resistance, promote cardiac efficiency, and maximize cellular oxygenation and organ protection.
- Avoid mechanical hyperventilation and allow spontaneous breathing whenever possible. Hyperventilation depletes CO2 tissue reserves, undermines respiratory drive, exaggerates opioid respiratory depression, and inhibits cardiac output, tissue perfusion, tissue oxygenation, and organ protection.
- Maintain pulse oximeter readings no higher than 89 by diluting the inhaled gas mixture with nitrogen or compressed air to minimize pulmonary oxygen toxicity and maintain effective hemoglobin saturation in blood emerging from the lung. Higher readings reflect meaningless plasma saturation with oxygen.
- Monitor the partial pressure of oxygen in peripheral tissues using transcutaneous O2/CO2 technology to confirm effective tissue oxygenation.
- Antibiotics as needed to control secondary bacterial infestations.
- General anesthesia with ½ MAC (minimal alveolar concentration) Isoflurane (about 1%) to prevent fear and anxiety that harmfully activates the “cognitive pathway” of the stress mechanism that generates fear and harmful sympathetic nervous activity.

- Supplement with intravenous magnesium sulphate using eclampsia protocols as needed to mitigate thrombin activity and control blood hypercoagulability.
- Avoid transfusions with packed red blood cells to treat mild or moderate anemia. The anemia beneficially promotes blood turbulence that inhibits harmful coagulopathy.
- Monitor blood coagulability using TEG or Viscoelastograph.
- Note: there is no clinically available antidote for tissue factor that can control the “tissue factor pathway” that activates the stress mechanism. The development of such a treatment would revolutionize health care.156
Long COVID Diagnosis
The available evidence, as illustrated by Susan’s case, suggests that the risk of DIC and Long COVID increases with each additional COVID immunization.39,115 The following tests may warn of dangerous hypercoagulability caused by COVID and its immunizations that can be treated with anticoagulants to prevent complications:
- Increased peripheral vascular resistance caused by arterial obstruction by abnormal clots and/or capillary obstruction by micro-emboli.157
- Thromboelastograph (TEG) is a sensitive test of blood hypercoagulability.
- Tissue biopsy can confirm inflammation of the vascular endothelium.
- Angiography may detect abnormal “calamari” strands of insoluble fibrin in arteries, and heart ventricles.68
- Elevated d-Dimer or FSP reflects capillary gate hyperactivity158
- Albuminuria reflects stress mechanism hyperactivity that disrupts the glycocalyx and releases albumen protein into the bloodstream.95-99
- Hyaline casts in the urine also reflect stress mechanism hyperactivity that causes soluble fibrin accumulation in glomeruli.
Long COVID Treatment
Anticoagulant therapy alleviates Long COVID symptoms.58 Streptokinase is the ideal anticoagulant choice for Long COVID because it has been extensively tested for human safety and effectiveness. It was regarded as a “miracle drug” for treatment of myocardial infarction, pulmonary embolus, and ischemic stroke in the 1980’s.159-162 Unfortunately, it was supplanted by coronary artery bypass surgery and angioplasty, and is no longer available in North America because it causes hypotension, which actually reflects its superior ability to disintegrate abnormal clots, open the capillary gate, reduce flow resistance, and restore microvascular perfusion.163,164 Fortunately, streptokinase remains available from its German manufacturer.165 Alternatives include urokinase,77,166-170 TPA (tissue plasminogen activator),171-174 Chelation therapy,175,176 Magnesium sulphate,177 and trisodium citrate.177,178
Management of DIC Caused By COVID Immunization
In the event that DIC is suspected, a simple and readily available CBC test can detect DIC anemia. Blood transfusion for moderate anemia should be avoided so as to allow blood turbulence to restore arterial patency and re-mobilize red cells removed from circulation by abnormal coagulation activity. Early treatment with streptokinase or other anticoagulant medications that activate plasminogen and promote restoration of red cells to circulation should be considered.

Discussion
The COVID contagion illustrates the explanatory power of the mammalian stress mechanism:
- It explains the pathological effects of COVID and its immunizations.
- It explains how the “novel” coronavirus causes viral pneumonia by attacking the pulmonary endothelium and provoking inflammation and exudates.
- It explains how the COVID contagion causes systemic inflammation that causes loss of smell, taste, and hair, and why older victims and those suffering obesity and chronic illnesses suffer greater COVID morbidity and mortality than younger victims.
- It explains why the mRNA vaccinations are more dangerous than COVID itself, and why repeated vaccinations progressively exaggerate the danger.
- Perhaps most interesting of all, it proposes a hitherto unrecognized form of DIC that causes unexpected sudden death in young, healthy victims without warning symptoms, and may provide a universal explanation of sudden death in a wide variety of circumstances such as earthquakes and other forms of severe stress and fright.179
Considering the following observations, it is difficult to avoid the conclusion that the COVID immunizations represent a novel form of genocide:
- There is no question that the “novel” coronavirus is a laboratory creation, because Scientific American announced that an American researcher and a Netherlands researcher simultaneously discovered the means to exaggerate coronavirus virulence in 2010.1,2 The researchers were immediately concerned that “terrorists” could abuse their discovery.
- The COVID contagion is reminiscent of Goldilocks and the three bears: it was preceded by the extremely lethal “SARS” (Severe Acute Respiratory Syndrome) contagion in China, followed by the somewhat less lethal “MERS” (Middle Eastern Respiratory Syndrome) that appeared in Iran and killed hundreds of citizens, and coronavirus epidemics in Chinese chickens and mink in the Netherlands. The porridge was too virulent in the SARS and MERS versions, and it didn’t successfully transfer from animals to people, but the COVID virulence was “just right.”
- Anthony Fauci issued urgent public warnings of the impending COVID epidemic even before it happened. His moral turpitude is obvious.
- Dr. Fauci’s mediocre scientific accomplishments were obfuscated by artificial “honors” (see Wikipedia).
- Governments around the world imposed drastic travel restrictions, curfews, quarantines, business closures, mask mandates and so forth. These measures arguably exaggerated the severity of the contagion by forcing people to live in crowded conditions. Countries like Sweden that ignored this nonsense enjoyed lower morbidity and mortality.
- As the contagion progressed, governments provided emergency subsidies for manufacturing mechanical ventilators that exaggerated the morbidity and mortality of the COVID contagion because of the harmful habit of hyperventilation that prevails throughout all fields of medicine.”180
- The new generation of mRNA “vaccines” were rushed into production without customary safety testing and made available free of charge via government subsidies.
- The American government illegally and unconstitutionally suppressed free speech by retaining Facebook, YouTube, and other private forums to squelch commentary by “anti-vaxxers,” despite increasing evidence that mRNA “vaccinations” cause more morbidity and mortality than COVID itself.41,51,111
- Laws were passed to declare that the new mRNA immunizations must be legally described as “vaccines” and special legal measures were imposed to make their manufacturers immune from lawsuits.
- Despite their dangers and lack of benefits, neither the government nor the pharmaceutical manufacturers has yet to halt the jabs.
- Perhaps most outrageous of all, this murderous COVID immunization campaign is being forced upon military personnel as well as civilians. The soldiers who are supposed to be defending us against our enemies are being murdered by their own commanders. It is difficult to imagine anything more deceitful and insane, because the military exemplifies national defense, which is the most fundamental purpose of government. One shudders to consider the implications for military morale.
Taken together with naturally declining fertility caused by prosperity, the combination of sudden deaths, miscarriages, and damaged fertility caused by the genocidal COVID contagion may ultimately devastate civilization, much like the bubonic plague that devastated Europe during the dark ages. Furthermore, it illustrates the power of corrupt corporations, whose owners and operatives are shielded from responsibility, to damage or even destroy civilization. History has consistently demonstrated that excessive concentrations of wealth and power portend the collapse of civilization from within, for no individual, nor even a small group of individuals, drunk with power and privilege, are capable of maintaining healthy debate, discussion, fairness, fair play, balance, and sanity that sustains healthy civilization.
Conclusion
Medicine is a social science, and politics is nothing else but medicine on a large scale. Medicine, as a social science, as the science of human beings, has the obligation to point out problems and to attempt their theoretical solution: the politician, the practical anthropologist, must find the means for their actual solution. The physicians are the natural attorneys of the poor, and social problems fall to a large extent within their jurisdiction.
—-Rudolf Virchow
Medicine has done its job: it has provided a theoretical solution to the dilemma of disease. The discovery of the mammalian stress mechanism represents the triumph of 20th century medical research, and it promises to become the next great advance in medical and biological theory. As long anticipated, it functions as the “companion mechanism” of DNA that converts the genetic blueprint into embryological development, and then remains active for the duration of life to repair tissues and regulate organs. It explains physiology, pathology, stress, and their relationships, and enables a “unified theory of medicine” that directs treatments at the cause of disease rather than its symptoms. It promises productive and profitable pharmacological development that will enable a new era of human existence, free from the eternal curse of disease and premature death.
The implications of the stress mechanism exceed the bounds of medicine. It confers a unified theory of biology that resolves the disparities of Darwin, Lamarck, Baldwin and Saltation. It explains embryology, evolution, ethology, extinction, longevity, taxonomy, anatomy, sex, speciation, the Cambrian explosion, and dinosaurs. The next great advances in medicine and biology will likely derive from artificial intelligence that deciphers presently inscrutable genetic information, and the discovery of mechanisms that convert chromosomal genetic information into PAR (thrombin) receptor configurations on the cell surface to enable embryological development and tissue repair.181-186 These advances will enable humans to control evolution, with implications that presently reside in the realm of science fiction.
The testing, confirmation, and implementation of the stress mechanism now lies in the hands of power, politics, privilege, and persuasion that prevails over all forms of human endeavor. My question is: Must these blessings await the arrival of our great-grandchildren? Why not us? Why not now?
References
1 Interlandi, J. Contagion: Controversy Erupts over Man-Made Pandemic Avian Flu Virus, <https://www.scientificamerican.com/article/contagion-controversy-erupts/> (2011).
2 Interlandi, J. A man-made contagion, <https://www.ncbi.nlm.nih.gov/pubmed/22295668> (2012).
3 Barry, J. M. The great influenza : the epic story of the deadliest plague in history. (Penguin Books, 2005).
4 Sutherland, S. Long COVID Now Looks like a Neurological Disease, Helping Doctors to Focus Treatments, <https://www.scientificamerican.com/article/long-covid-now-looks-like-a-neurological-disease-helping-doctors-to-focus-treatments/> (2023).
5 Bergamaschi, G. et al. Anemia in patients with Covid-19: pathogenesis and clinical significance. Clin Exp Med 21, 239-246 (2021). https://doi.org:10.1007/s10238-020-00679-4
6 Schilling, R. F., Gangnon, R. E. & Traver, M. Arteriosclerotic events are less frequent in persons with chronic anemia: evidence from families with hereditary spherocytosis. Am J Hematol 81, 315-317 (2006).
7 Whoriskey, P. Anemia drug made billions, but at what cost?, <https://www.washingtonpost.com/business/economy/anemia-drug-made-billions-but-at-what-cost/2012/07/19/gJQAX5yqwW_story.html> (July 19, 2012).
8 Yoon, H. et al. The relationship between anemia and pulse pressure and hypertension: The Korea National Health and Nutrition Examination Survey 2010-2012. Clin Exp Hypertens 40, 650-655 (2018). https://doi.org:10.1080/10641963.2017.1416123
9 Levy, T. E. Myocarditis: Once Rare, Now Common, <https://www.theepochtimes.com/health/myocarditis-once-rare-now-common_5060101.html?utm_source=newsnoe&src_src=newsnoe&utm_campaign=breaking-2023-02-17-one&src_cmp=breaking-2023-02-17-one&utm_medium=email&est=piW8HSBqDmPVYcHfsBitemoNgC2vt6sjsKMZlNQaNC4V5S2%2FHitHwdcuL6pBBYP5> (2023).
10 Lefringhausen2, C. T. a. A. COVID-19 vaccines – An Australian Review. Journal of Clinical & Experimental Immunology 7, 491-508 (2022 September).
11 Robert Malone, D. O. R. Medical Countermeasures Analysis of 2019-nCoV and Vaccine Risks for Antibody-Dependent Enhancement (ADE), <https://www.researchgate.net/publication/340149846_Medical_Countermeasures_Analysis_of_2019-nCoV_and_Vaccine_Risks_for_Antibody-Dependent_Enhancement_ADE> (January 2020).
12 Robert W. Malone, M., MS; Dr. Ryan Cole, MD; Lynn Flynn, MD; Dr. Richard Urso; Dr. Harvey Risch MD, PhD; Brian Tyson, MD; Peter McCollough, MD, MPH; Kirk Milhoan, MD, PhD; Lynn Fynn, MD; David Wisesman, PhD, MRPharmS; Mary Talley Bowden, MD Stanford trained otolaryngologist and sleep medicine specialist; Fadt Hannah-Shmouni, MD, FRCPC; Michael Yeadon, PhD; . Global COVID Summit, <https://rwmalonemd.substack.com/p/power-and-strategy-of-false-narratives> (October 3, 2022).
13 Dong, A. K. D. Y. Booster Shots May Trigger Stroke Incidents, According to CDC and FDA, <https://www.theepochtimes.com/health/booster-shots-may-trigger-stroke-incidents-according-to-cdc-and-fda_5021604.html?utm_source=morningbriefnoe&src_src=morningbriefnoe&utm_campaign=mb-2023-02-13&src_cmp=mb-2023-02-13&utm_medium=email&est=VgFVsGNyD%2BPAIq%2FmfyL%2BSHW5QpJsTt7c1EovS%2Bcn8ciB7BFZl5u2yZnQIqAm3Yvr> (2023 February 11).
14 Ellis, R. Possible Bivalent Vaccine Link to Strokes in People Over 65, <https://www.medscape.com/viewarticle/987016?src=mkm_ret_230131_mscpmrk-GB_ExcNews_MDHC&uac=264431HV&impID=5118805&faf=1> (2023, January 17).
15 Expose, T. UK Government confirms COVID Vaccines are deadly as they reveal Mortality Rates per 100k are lowest among the Unvaccinated in all Age Groups, <https://expose-news.com/2022/08/09/mortality-rates-lowest-among-unvacinated/?utm_source=substack&utm_medium=email> (2023).
16 Fraiman, J. et al. Serious adverse events of special interest following mRNA COVID-19 vaccination in randomized trials in adults. Vaccine 40, 5798-5805 (2022). https://doi.org:10.1016/j.vaccine.2022.08.036
17 Hohman, M. Since COVID, more young people are dying of heart attacks. Here’s what we know, <https://www.today.com/health/covid-heart-attack-young-people-rcna69903> (2023 February 9).
18 Hryniewicki, A. T., Tolia, V. M. & Nene, R. V. Cardiac Tamponade After COVID-19 Vaccination. J Emerg Med 62, 250-253 (2022). https://doi.org:10.1016/j.jemermed.2021.10.008
19 John Stirling, I. e. Top Insurance Analyst Finds 7% Increase In Mortality for Each Covid Vax Dose Received, <https://needtoknow.news/2023/02/top-insurance-analyst-finds-7-increase-in-mortality-for-each-covid-vax-dose-received/?utm_source=substack&utm_medium=email> (2023).
20 Kirsch, S. Bhakdi/Burkhardt pathology results show 93% of people who died after being vaccinated were killed by the vaccine, <https://stevekirsch.substack.com/p/bhakdiburkhardt-pathology-results> (2021).
21 Macias Saint-Gerons, D., Ibarz, M. T., Castro, J. L., Fores-Martos, J. & Tabares-Seisdedos, R. Myopericarditis Associated with the Novavax COVID-19 Vaccine (NVX-CoV2373): A Retrospective Analysis of Individual Case Safety Reports from VigiBase. Drugs Real World Outcomes, 1-8 (2023). https://doi.org:10.1007/s40801-023-00355-5
22 Mercola, D. J. COVID Boosters Trigger Metastasis, <https://articles.mercola.com/sites/articles/archive/2023/01/05/covid-boosters-trigger-metastasis.aspx?ui=063ac0a92006e5012244a16187dd09023089107133e97a24b565285d1ef47e90&sd=20220103&cid_source=dnl&cid_medium=email&cid_content=art1HL&cid=20230105&cid=DM1321022&bid=1686965054> (2023, January 5).
23 Mungmunpuntipantip, R. & Wiwanitkit, V. Acute venous thromboembolism after COVID-19 vaccination. J Vasc Surg Venous Lymphat Disord 10, 285 (2022). https://doi.org:10.1016/j.jvsv.2021.08.024
24 News, R. E. C. Alberta has seen roughly 10,000 ‘excess’ deaths since 2020, and COVID doesn’t explain it all, <https://www.cbc.ca/news/canada/calgary/excess-deaths-alberta-1.6731344?utm_source=substack&utm_medium=email> (2023 February 2).
25 Nie, X. et al. Multi-organ proteomic landscape of COVID-19 autopsies. Cell 184, 775-791 e714 (2021). https://doi.org:10.1016/j.cell.2021.01.004
26 Parpia, R. High Blood Pressure After COVID Shots Not So Rare, <https://thevaccinereaction.org/2023/01/high-blood-pressure-after-covid-shots-not-so-rare/?utm_source=substack&utm_medium=email> (2023 January 30).
27 Rennick, G. Australian Senator Takes Hard Stand Against COVID Jabs, <https://articles.mercola.com/sites/articles/archive/2022/12/29/australian-senator-against-covid-jabs.aspx?ui=063ac0a92006e5012244a16187dd09023089107133e97a24b565285d1ef47e90&sd=20220103&cid_source=dnl&cid_medium=email&cid_content=art1ReadMore&cid=20221229&cid=DM1315988&bid=1681242027> (2022).
28 Richard, L. Elon Musk felt like he ‘was dying’ after 2nd COVID booster shot, cousin in ‘peak health’ suffered myocarditis, <https://www.foxbusiness.com/business-leaders/elon-musk-felt-like-he-was-dying-2nd-covid-booster-shot-cousin-peak-health-suffered-myocarditis> (2023, January 21).
29 Rishma Par, m. Thousands of Cases of Pulmonary Embolism Reported After COVID Shots, <https://thevaccinereaction.org/2023/02/thousands-of-cases-of-pulmonary-embolism-reported-after-covid-shots/> (2023 February 5).
30 Sanada, Y., Azuma, J., Hirano, Y., Hasegawa, Y. & Yamamoto, T. Overlapping Myocarditis and Postural Orthostatic Tachycardia Syndrome After COVID-19 Messenger RNA Vaccination: A Case Report. Cureus 14, e31006 (2022). https://doi.org:10.7759/cureus.31006
31 Singh, P. & Schwartz, R. A. Disseminated intravascular coagulation: A devastating systemic disorder of special concern with COVID-19. Dermatol Ther 33, e14053 (2020). https://doi.org:10.1111/dth.14053
32 Sinha, S. & Tripathy, S. COVID-19 Vaccine-associated Thrombosis (Disseminated Intravascular Thrombosis) with Rare Cutaneous Involvement. Indian J Crit Care Med 26, 963-965 (2022). https://doi.org:10.5005/jp-journals-10071-24282
33 Spinney, L. What Long Flu Sufferers of the 1918-1919 Pandemic Can Tell Us About Long COVID Today, <https://time.com/5915616/long-flu-1918-pandemic/> (2020, December 31).
34 Stat, C. DIC in COVID-19—Insights From the Front Lines, <https://www.aacc.org/cln/cln-stat/2020/june/4/disseminated-intravascular-coagulation-in-covid-19-insights-from-the-front-lines> (2020).
35 Sy. Australian COVID-19 pandemic: A Bradford Hill analysis of iatrogenic excess mortality, <https://www.researchgate.net/publication/368426122_Australian_COVID-19_pandemic_A_Bradford_Hill_analysis_of_iatrogenic_excess_mortality> (2023).
36 Thachil, J. COVID-19 Vaccine-Induced Immune Thrombosis with Thrombocytopenia (VITT) and the Shades of Grey in Thrombus Formation. Semin Thromb Hemost 48, 15-18 (2022). https://doi.org:10.1055/s-0041-1735453
37 Tilley, C. in Daily Mail https://www.dailymail.co.uk/health/article-11466261/Majority-Covid-deaths-vaccinated-Americans-time.html (Daily Mail, London, 2022).
38 Tomás M. León, P. V. D., PhD2; Lauren Nelson, MPH1; Emily Lutterloh, MD2,3; Ursula E. Bauer, PhD2; Bryon Backenson, MPH2,3; Mary T. Bassett, MD2; Hannah Henry, MPH1; Brooke Bregman, MPH1; Claire M. Midgley, PhD4; Jennifer F. Myers, MPH1; Ian D. Plumb, MBBS4; Heather E. Reese, PhD4; Rui Zhao, MPH1; Melissa Briggs-Hagen, MD4; Dina Hoefer, PhD2; James P. Watt, MD1; Benjamin J. Silk, PhD4; Seema Jain, MD1; Eli S. Rosenberg, PhD2,3. COVID-19 Cases and Hospitalizations by COVID-19 Vaccination Status and Previous COVID-19 Diagnosis — California and New York, May–November 2021, <https://www.cdc.gov/mmwr/volumes/71/wr/mm7104e1.htm?utm_source=substack&utm_medium=email> (2022 January 28).
39 Wahl, M. Z. a. L. Report 48: VAERS – 76% of Vaccine-Related Miscarriages from the Past 30 Years Occurred Once Pregnant Women Started Receiving COVID-19 Vaccines, <https://dailyclout.io/miscarriages-in-covid-19-vaccinated-mothers-as-reported-in-vaers/?utm_source=substack&utm_medium=email> (2022 December 1).
40 Yamamoto, K. Adverse effects of COVID-19 vaccines and measures to prevent them. Virol J 19, 100 (2022). https://doi.org:10.1186/s12985-022-01831-0
41 Dowd, E. Cause Unknown: The Epidemic of Sudden Deaths in 2021 and 2022. 216 (Skyhorse, 2022, December 13).
42 Vossoughian, Y. Yasmin on her Health Scare, <https://www.msnbc.com/yasmin-vossoughian/watch/yasmin-vossoughian-opens-up-about-health-scare-162059333658?utm_source=substack&utm_medium=email> (2023, January 28).
43 Patone, M. et al. Risks of myocarditis, pericarditis, and cardiac arrhythmias associated with COVID-19 vaccination or SARS-CoV-2 infection. Nature medicine 28, 410-422 (2022). https://doi.org:10.1038/s41591-021-01630-0
44 Novak, A. Damar Hamlin may have suffered “remarkably rare” condition, Dr. Agus says, <https://www.cbsnews.com/news/damar-hamlin-buffalo-bills-condition-injury-cardiac-arrest/> (2022).
45 Kulick, D. An EMT’s take on Damar Hamlin’s cardiac arrest | Something to Think About, 2023).
46 News, B. Buffalo Bills Release Statement on What Actually Happened to Damar Hamlin, <https://beckernews.com/buffalo-bills-release-statement-on-what-actually-happened-to-damar-hamlin-48365/> (January 3, 2023).
47 Gill, J. R., Tashjian, R. & Duncanson, E. Autopsy Histopathologic Cardiac Findings in 2 Adolescents Following the Second COVID-19 Vaccine Dose. Arch Pathol Lab Med 146, 925-929 (2022). https://doi.org:10.5858/arpa.2021-0435-SA
48 Schwab, C. et al. Autopsy-based histopathological characterization of myocarditis after anti-SARS-CoV-2-vaccination. Clin Res Cardiol, 1-10 (2022). https://doi.org:10.1007/s00392-022-02129-5
49 Cole, D. R. Shocking Lab Investigation of COVID Vaccines, <https://takecontrol.substack.com/p/lab-investigation-covid-vaccines> (2022).
50 Varga, Z. et al. Endothelial cell infection and endotheliitis in COVID-19. Lancet 395, 1417-1418 (2020). https://doi.org:10.1016/S0140-6736(20)30937-5
51 Doolan, A., Langlois, N. & Semsarian, C. Causes of sudden cardiac death in young Australians. Med J Aust 180, 110-112 (2004).
52 Mercola, D. J. Banking on a Shot in the Dark, <https://takecontrol.substack.com/p/banking-on-a-shot-in-the-dark> (2022).
53 News, T. S. New Zealand Study: Pfizer’s mRNA Vaccine Statistically Significant Link to Myocarditis, <https://www.youtube.com/watch?v=QAaTxU8Eg_o> (
54 steve-kirsch. The FAA has very quietly tacitly admitted that the EKGs of pilots are no longer normal. We should be concerned. Very concerned., <https://stevekirsch.substack.com/p/the-faa-has-very-quietly-tacitly> (2023).
55 Hisle, J. in The Epoch Times (2023, January 23).
56 Chasco, E. E. et al. Brain Fog and Fatigue following COVID-19 Infection: An Exploratory Study of Patient Experiences of Long COVID. Int J Environ Res Public Health 19 (2022). https://doi.org:10.3390/ijerph192315499
57 Mansell, V., Hall Dykgraaf, S., Kidd, M. & Goodyear-Smith, F. Long COVID and older people. Lancet Healthy Longev 3, e849-e854 (2022). https://doi.org:10.1016/S2666-7568(22)00245-8
58 Medinger, G. How to Treat “Microclots” in Long Covid With Dr. Jaco Laubscher, <https://www.youtube.com/watch?v=vWisaTFp4KI&t=5s> (2022).
59 Saini, G. & Aneja, R. Cancer as a prospective sequela of long COVID-19. Bioessays 43, e2000331 (2021). https://doi.org:10.1002/bies.202000331
60 Waade, M. DR. RYAN COLE: THE DANGERS OF COVID-19 SHOTS SPIKE PROTEINS FROM WILDFIRE CANCERS TO FOOT-LONG CLOTS, <https://www.bitchute.com/video/A4qFrwmGeMBE/> (2023).
61 Woleben, H. R. US death-benefit payouts hit record high in 2021, <https://www.spglobal.com/marketintelligence/en/news-insights/latest-news-headlines/us-death-benefit-payouts-hit-record-high-in-2021-69102708> (2022, March 15).
62 Devitt, M. CDC Data Show U.S. Life Expectancy Continues to Decline, <https://www.aafp.org/news/health-of-the-public/20181210lifeexpectdrop.html> (2018).
63 Katella, K. Omicron and the BQs: A Guide to What We Know. Experts monitor the data as new strains emerge (2022). <https://www.yalemedicine.org/news/5-things-to-know-omicron>.
64 Dowling, M. The Sad Sudden Death of Uche Nwaneri, <https://www.independentsentinel.com/the-sad-sudden-death-of-uche-nwaneri/> (2023).
65 Ganz, J. ‘Triangle of Sadness’ star Charlbi Dean, 32, died of rare infection, <https://news.yahoo.com/triangle-sadness-star-charlbi-dean-180200181.html> (2022).
66 Mazumdar., T. Charlbi Dean’s Death: Actress’ Brother Dubs Antivax Theory ‘Completely Ridiculous’, <https://www.ibtimes.com/charlbi-deans-death-actress-brother-dubs-antivax-theory-completely-ridiculous-3608095> (2022).
67 Novelly, T. Air Force Academy Cadet Dies Suddenly While Walking to Class, <https://www.military.com/daily-news/2023/01/11/air-force-academy-cadet-dies-suddenly-while-walking-class.html> (2023).
68 Peters, S. (ed Steward Peters) https://rumble.com/v1wac7i-world-premier-died-suddenly.html (Joseph Mercola, 2022).
69 Peterson, J. (ed Jordan Peterson) https://www.youtube.com/watch?v=FEh5JyZC218 (AUDIBLE.COM, 2022).
70 Thapa, R. et al. Post-Coronavirus disease syndrome (post-COVID-19) syndrome: A case report. Clin Case Rep 10, e6719 (2022). https://doi.org:10.1002/ccr3.6719
71 Proal, D. A. Interview with Dr. Akiko Iwasaki: An overview of her research on LongCovid and ME/CFS, <https://www.youtube.com/watch?v=TJwUi4p9JHc> (2022).
72 Pezzullo, A. M., Axfors, C., Contopoulos-Ioannidis, D. G., Apostolatos, A. & Ioannidis, J. P. A. Age-stratified infection fatality rate of COVID-19 in the non-elderly population. Environ Res 216, 114655 (2023). https://doi.org:10.1016/j.envres.2022.114655
73 Fakhoury, H. M. A. et al. Lung-Centric Inflammation of COVID-19: Potential Modulation by Vitamin D. Nutrients 13 (2021). https://doi.org:10.3390/nu13072216
74 Heubel, A. D. et al. Determinants of endothelial dysfunction in noncritically ill hospitalized COVID-19 patients: A cross-sectional study. Obesity (Silver Spring) (2021). https://doi.org:10.1002/oby.23311
75 Dowd, E. “Cause Unknown” The Epidemic of sudden Deaths in 2021 and 2022. (Skyhorse Publishing, 2022).
76 Wikipedia. Spanish Flu, <https://en.wikipedia.org/wiki/Spanish_flu> (
77 Idell, S. Endothelium and disordered fibrin turnover in the injured lung: newly recognized pathways. Critical care medicine 30, S274-280 (2002).
78 Colunga Biancatelli, R. M. L. et al. The SARS-CoV-2 spike protein subunit S1 induces COVID-19-like acute lung injury in Kappa18-hACE2 transgenic mice and barrier dysfunction in human endothelial cells. Am J Physiol Lung Cell Mol Physiol 321, L477-L484 (2021). https://doi.org:10.1152/ajplung.00223.2021
79 Mercola, J., Cummins, R. & Kennedy, R. F. The truth about COVID-19 : exposing the great reset, lockdowns, vaccine passports, and the new normal. (Chelsea Green Publishing ;
Somerest House, 2021).
80 Kuhn, T. S. & Hacking, I. The structure of scientific revolutions. Fourth edition. edn, (The University of Chicago Press, 2012).
81 Coleman, L. S. A Stress Repair Mechanism that Maintains Vertebrate Structure during Stress. Cardiovasc Hematol Disord Drug Targets (2010). https://doi.org:BSP/CHDDT/E-Pub/00015 [pii]
82 Coleman, L. A Hypothesis: Factor VII governs clot formation, tissue repair and apoptosis. Medical Hypotheses in press (2007).
83 Coleman, L. S. in 50 Years Lost in Medical Advance (ed Jeffrey Walden) https://www.youtube.com/watch?v=efi9v86isSw&t=117s (YouTube, YouTube, 2022).
84 Coleman, L. S. A capillary hemostasis mechanism regulated by sympathetic tone and activity via factor VIII or von Willebrand’s factor may function as a “capillary gate” and may explain angiodysplasia, angioneurotic edema, and variations in systemic vascular resistance. Med Hypotheses (2005).
85 Coleman, L. S. Stress repair mechanism activity explains inflammation and apoptosis. Advances in Bioscience and Biotechnology 3, 459-503 (2012). https://doi.org:10.4236/abb.2012.324065
86 Fleck, R. A., Rao, L. V., Rapaport, S. I. & Varki, N. Localization of human tissue factor antigen by immunostaining with monospecific, polyclonal anti-human tissue factor antibody. Thromb Res 59, 421-437 (1990).
87 Coleman, L. S. An Improved Explanation of Atherosclerosis. PLoS Medicine 2(4):e98 (2005).
88 Coleman, L. S. Insoluble fibrin may reduce turbulence and bind blood components into clots. Med Hypotheses 65, 820-821 (2005).
89 Coleman, L. S. A testable hypothesis that may explain the morbidity and mortality caused by surgical stress. Anesth Analg 103, 1589; author reply 1589-1590 (2006).
90 Coleman, L. S. To the Editor: Is von Willebrand Factor a Hormone that Regulates a Coagulation Mechanism? World J Surg (2006).
91 Coleman, L. S. Atherosclerosis may be caused by inadequate levels of turbulence and mixing. World J Surg 30, 638-639 (2006).
92 Coleman, L. S. A Testable Stress Mechanism Explains Both Unified Stress Theory and Capillary Gate Theory. FDA Anesthesia & Life Support Drugs Advisory Committee pp239-243 3/29/07 (2007).
93 Coleman, L. S. A Hypothesis: Factor VII governs clot formation, tissue repair and apoptosis. Medical Hypotheses in press (2007).
94 Coleman, L. S. 50 Years Lost in Medical Advance: The Discovery of Hans Selye’s Stress Mechanism. (The American Institute of Stress Press, 2021).
95 Chappell, D., Jacob, M., Hofmann-Kiefer, K., Conzen, P. & Rehm, M. A rational approach to perioperative fluid management. Anesthesiology 109, 723-740 (2008).
96 Ono, S., Egawa, G. & Kabashima, K. Regulation of blood vascular permeability in the skin. Inflamm Regen 37, 11 (2017). https://doi.org:10.1186/s41232-017-0042-9
97 Reitsma, S., Slaaf, D. W., Vink, H., van Zandvoort, M. A. & oude Egbrink, M. G. The endothelial glycocalyx: composition, functions, and visualization. Pflugers Arch 454, 345-359 (2007). https://doi.org:10.1007/s00424-007-0212-8
98 Sukhikh, G. T. et al. Differences of glycocalyx composition in the structural elements of placenta in preeclampsia. Placenta 43, 69-76 (2016). https://doi.org:10.1016/j.placenta.2016.05.002
99 Ziganshina, M. M., Pavlovich, S. V., Bovin, N. V. & Sukhikh, G. T. Hyaluronic Acid in Vascular and Immune Homeostasis during Normal Pregnancy and Preeclampsia. Acta Naturae 8, 59-71 (2016).
100 Rath, W., Faridi, A. & Dudenhausen, J. W. HELLP syndrome. J Perinat Med 28, 249-260 (2000).
101 Tous, M. et al. Circulating blood cells modulate the atherosclerotic process in apolipoprotein E-deficient mice. Metabolism: clinical and experimental 53, 95-100 (2004).
102 Smith, K. J., Bleyer, A. J., Little, W. C. & Sane, D. C. The cardiovascular effects of erythropoietin. Cardiovascular Research 59, 538-548 (2003). https://doi.org:S0008636303004681 [pii]
103 Siddique, H. Blood doping: what is it and has anyone died as a result of it?, <https://www.theguardian.com/sport/2015/aug/02/blood-doping-what-is-it-and-has-anyone-died-as-a-result-of-it> (2015).
104 Brimble, K. S., McFarlane, A., Winegard, N., Crowther, M. & Churchill, D. N. Effect of chronic kidney disease on red blood cell rheology. Clin Hemorheol Microcirc 34, 411-420 (2006).
105 Dunne, J. R., Malone, D., Tracy, J. K., Gannon, C. & Napolitano, L. M. Perioperative anemia: an independent risk factor for infection, mortality, and resource utilization in surgery. J Surg Res 102, 237-244 (2002).
106 Fernandez, F. et al. Low haematocrit and prolonged bleeding time in uraemic patients: effect of red cell transfusions. British journal of haematology 59, 139-148 (1985).
107 Mansanguan, S. et al. Cardiovascular Manifestation of the BNT162b2 mRNA COVID-19 Vaccine in Adolescents. Trop Med Infect Dis 7 (2022). https://doi.org:10.3390/tropicalmed7080196
108 Becker, K. New Swiss Study: Covid Shots Increase Risk of Myocarditis by 800 TIMES in Young Adults, <https://beckernews.com/new-swiss-study-covid-shots-increase-risk-of-myocarditis-by-800-times-in-young-adults-47674/?utm_source=substack&utm_medium=email> (2022, October 29).
109 George, J. Functional Neurological Disorder Emerges After COVID Infection, Vaccines, <https://www.medpagetoday.com/neurology/longcovid/103708?utm_source=substack&utm_medium=email> (2023, March 24).
110 Board, P. E. New York’s kid-vaccination collapse is a grim result of ‘expert’ COVID misinfo, <https://nypost.com/2023/02/05/new-yorks-kid-vaccination-collapse-is-a-grim-result-of-expert-covid-misinfo/?utm_source=substack&utm_medium=email> (2023 February 5).
111 Carolyn Hendler, J. Post COVID Vaccine Heart-Related Deaths Sharply Increase, Especially in Young Males, <https://thevaccinereaction.org/2023/03/post-covid-vaccine-heart-related-deaths-sharply-increase-especially-in-young-males/> (2023).
112 Warr, T. A., Rao, L. V. & Rapaport, S. I. Disseminated intravascular coagulation in rabbits induced by administration of endotoxin or tissue factor: effect of anti-tissue factor antibodies and measurement of plasma extrinsic pathway inhibitor activity. Blood 75, 1481-1489 (1990).
113 Asakura, H. & Ogawa, H. COVID-19-associated coagulopathy and disseminated intravascular coagulation. Int J Hematol 113, 45-57 (2021). https://doi.org:10.1007/s12185-020-03029-y
114 Bhakdi, S. Thai Princess coma mystery – world expert says it’s a COVID jab injury, <https://www.theburningplatform.com/2023/02/04/thai-princess-coma-mystery-world-expert-says-its-a-covid-jab-injury/> (2023 February 4).
115 Nigh2, S. S. a. G. Worse Than the Disease? Reviewing Some Possible Unintended Consequences of the mRNA Vaccines Against COVID-19. International Journal of Vaccine Theory, Practice, and Research https://doi.org/10.56098/ijvtpr.v2i1 (2021 May 10).
116 Sports, M. B. s. T. H. S. Buffalo Bills vs Cincinnati Bengals RAW BROADCAST includes the entire ESPN broadcast and reaction to Damar Hamlin injury, <https://www.youtube.com/watch?v=ZcqAfpZ_Jpg> (2023).
117 Uggetti, P. Caddie collapses, given CPR during AT&T Pebble Beach Pro-Am, <https://www.espn.com/golf/story/_/id/35584036/caddie-collapses-given-cpr-att-pebble-beach-pro-am> (2023 February 3).
118 Bader, F., Manla, Y., Atallah, B. & Starling, R. C. Heart failure and COVID-19. Heart Fail Rev 26, 1-10 (2021). https://doi.org:10.1007/s10741-020-10008-2
119 Liu, J., Deswal, A. & Khalid, U. COVID-19 myocarditis and long-term heart failure sequelae. Curr Opin Cardiol 36, 234-240 (2021). https://doi.org:10.1097/HCO.0000000000000832
120 Chen, L. et al. Ultrasound Imaging Findings of Acute Testicular Infection in Patients With Coronavirus Disease 2019: A Single-Center-Based Study in Wuhan, China. J Ultrasound Med 40, 1787-1794 (2021). https://doi.org:10.1002/jum.15558
121 Musk, E. ‘Felt Like I Was Dying for Several Days’: Elon Musk Says About Covid Booster, <https://news.yahoo.com/m/d65d9002-b470-3a8a-b34a-5e2ae62e767b/-felt-like-i-was-dying-for.html> (2023).
122 Medinger, G. Is THIS What’s Causing Long Covid?, <https://www.youtube.com/watch?v=94ZYVxtdNHY> (November 12, 2020).
123 Coleman, L. S. The Longevity Crisis, <https://www.stress.org/the-longevity-crisis> (2022).
124 Holemans, R. Enhancement of Fibrinolysis in the Dog by Injection of Vasoactive Drugs. The American journal of physiology 208, 511-520 (1965).
125 Takahashi, T., Suzukawa, M., Akiyama, M., Hatao, K. & Nakamura, Y. Systemic AL amyloidosis with disseminated intravascular coagulation associated with hyperfibrinolysis. Int J Hematol 87, 371-374 (2008). https://doi.org:10.1007/s12185-008-0070-y
126 Genovese, A. et al. Inhibition of hypoxia-induced cardiac hypertrophy by verapamil in rats. Basic Res Cardiol 75, 757-763 (1980).
127 Genovese, A., Chiariello, M., Latte, S., DeAlfieri, W. & Condorelli, M. Bilateral ventricular hypertrophy in rats exposed to acute or chronic hypobaric hypoxia. Respiration 44, 289-293 (1983).
128 Genovese, A., De Alfieri, W., Latte, S., Chiariello, M. & Condorelli, M. Regression of myocardial hypertrophy in the rat following removal of acute or chronic hypobaric hypoxia. Eur Heart J 3 Suppl A, 161-164 (1982).
129 Genovese, A., Latte, S., Bozzaotre, M. & Chiariello, M. Response of the left ventricular connective tissue to hypoxia. Res Exp Med (Berl) 183, 111-115 (1983).
130 Coleman, L. S. The Mammalian Stress Mechanism (MSM) Explains Radial Artery Spasm (RAS). J Anes Surg 5, 81-94 (2018). https://doi.org:10.15436/2377-1364.18.1870
131 Laubscher, J. in How To Treat “Microclots” in Long Covid (ed Gez Medinger) (Gez Medinger, https://www.youtube.com/watch?v=vWisaTFp4KI&t=5s, 2022).
132 Peters, S. www.bek.news/stewpetersshow/2022-2011-2021/ (BEK TV, 2022).
133 Schaller, T. et al. Postmortem Examination of Patients With COVID-19. JAMA (2020). https://doi.org:10.1001/jama.2020.8907
134 Morris, C. in redacted with Clayton Morris (ed Clayton Morris) (2023, February 4).
135 Alexander, D. P. American Airlines pilot Bob Snow suffered heart attack 6 minutes after he landed plane with 200 passengers on board; he is speaking out i)FAA no one contacted him ii) likely due to the vaccine, <https://twitter.com/healthbyjames/status/1620778219774566401?utm_source=substack&utm_medium=email> (2023 February 3).
136 Hisle, J. FAA Change to Heart-Test Limit Triggers Worries Over Pilot Health, Public Safety, <https://yournews.com/2023/01/24/2498918/faa-change-to-heart-test-limit-triggers-worries-over-pilot-health/> (2023 January 24).
137 Robert F. Kennedy, J. RFK, Jr. to Buttigieg: Airline Safety Is ‘Not a Partisan Issue,’ FAA Must Investigate Spike in Pilot Health Emergencies, <https://childrenshealthdefense.org/defender/rfk-jr-pete-buttigieg-pilot-health-airline-safety/?utm_source=luminate&utm_medium=email&utm_campaign=defender&utm_id=20230329> (2023).
138 Makis, D. W. Virgin Australia flight from Adelaide to Perth forced to make emergency landing as First Officer suffered heart attack 30 minutes after departure on March 3, 2023. (2023 March 3).
139 Moyes, S. BA TRAGEDY Veteran British Airways pilot collapses and dies shortly before he was due to captain packed passenger jet, <https://makismd.substack.com/p/veteran-british-airways-pilot-collapses?utm_source=substack&utm_medium=email> (2023, March 3).
140 Makis, D. W. Emirates Flight EK205 MXP-JFK from Milan diverted on March.13, 2023 due to pilot illness, returned to Milan for emergency landing – now 4th pilot incident this month. COVID Intel (2023, March 14).
141 Loh, C. First Officer Incapacitated During Air Transat Airbus A321 Flight, <https://simpleflying.com/first-officer-incapacitated-air-transat-a321-flight/> (2023 March 18).
142 Makis, D. W. TAROM Flight RO-7673 TSR-HRG service from Timisoara (Romania) to Hurghada (Egypt) diverted: 30 year old pilot had chest pain and collapsed in-flight on March 25th, 2023 – 7th pilot incident this month, <https://makismd.substack.com/p/tarom-flight-ro-7673-tsr-hrg-service?utm_source=substack&utm_campaign=post_embed&utm_medium=email> (2023, March 28).
143 J, C. Franco Harris Promoting the Jab, <https://www.youtube.com/watch?v=uEc48RUQJ3A> (2023).
144 Shaffer, D. C. a. J. Ravens player Jaylon Ferguson died of fentanyl and cocaine, medical examiner office says, <https://www.baltimoresun.com/maryland/baltimore-city/bs-md-ci-jaylon-ferguson-ravens-20220701-nii2vx7mofestog2cwdool5pbq-story.html> (2022, July 1).
145 D’Cunha, C. Riddick Parker death: Patriots Super Bowl winner dies at 49 after collapsing during bicycle ride, <https://www.sportskeeda.com/nfl/news-riddick-parker-death-patriots-super-bowl-winner-dies-49-collapsing-bicycle-ride> (2022, November 8).
146 Carlin, S. Rams LT Alaric Jackson to miss rest of season with blood clots, <https://theramswire.usatoday.com/2022/11/15/rams-alaric-jackson-out-for-season-blood-clots/> (2022, November 15).
147 Cannizzaro, M. Jets’ Max Mitchell dealing with blood clots: ‘Unexpected temporary setback’, <https://nypost.com/2022/12/08/jets-max-mitchell-out-for-season-while-dealing-with-blood-clots/> (2022).
148 Newton, D. Panthers’ Henry Anderson had stroke in Oct., now ready to play, <https://www.espn.com/nfl/story/_/id/35205784/panthers-henry-anderson-had-stroke-oct-now-ready-play> (2022, December 7).
149 Jessie Lemonier: Former Detroit Lions linebacker dies aged 25. (2023, January 26).
150 Argano, C. et al. Protective Effect of Vitamin D Supplementation on COVID-19-Related Intensive Care Hospitalization and Mortality: Definitive Evidence from Meta-Analysis and Trial Sequential Analysis. Pharmaceuticals (Basel) 16 (2023). https://doi.org:10.3390/ph16010130
151 Blondon, M. et al. Thrombin generation and fibrin clot structure after vitamin D supplementation. Endocr Connect 8, 1447-1454 (2019). https://doi.org:10.1530/EC-19-0429
152 Devereux, G. et al. Maternal vitamin D intake during pregnancy and early childhood wheezing. The American journal of clinical nutrition 85, 853-859 (2007).
153 EffSaliba, W., Awad, K., Ron, G. & Elias, M. The Effect of Vitamin D Supplementation on Thrombin Generation Assessed by the Calibrated Automated Thrombogram. Clin Appl Thromb Hemost 22, 340-345 (2016). https://doi.org:10.1177/1076029614556745
154 Shah Alam, M., Czajkowsky, D. M., Aminul Islam, M. & Ataur Rahman, M. The role of vitamin D in reducing SARS-CoV-2 infection: An update. Int Immunopharmacol 97, 107686 (2021). https://doi.org:10.1016/j.intimp.2021.107686
155 MARTÍN, C. S. S. The Plague of Athens killed tens of thousands, but its cause remains a mystery, <https://www.nationalgeographic.co.uk/history-and-civilisation/2021/05/the-plague-of-athens-killed-tens-of-thousands-but-its-cause-remains-a-mystery> (2021 May 21).
156 Welty-Wolf, K. E. et al. Coagulation blockade prevents sepsis-induced respiratory and renal failure in baboons. American journal of respiratory and critical care medicine 164, 1988-1996 (2001).
157 Morise, T. et al. Noninvasive, continuous evaluation of peripheral vascular resistance in humans. Hypertens Res 23, 15-19 (2000). https://doi.org:10.1291/hypres.23.15
158 Wada, H. et al. Increased soluble fibrin in plasma of patients with disseminated intravascular coagulation. Clin Appl Thromb Hemost 9, 233-240 (2003).
159 Neuhof H, H. D., Glaser E, Wolf H, Lasch H.G. Streptokinase Therapy in Patients with Acute Myocardial Infarction. Intensive Care Medicine Volume 1, 27-30 (1975).
160 Sikri, N. & Bardia, A. A history of streptokinase use in acute myocardial infarction. Tex Heart Inst J 34, 318-327 (2007).
161 Smith, B. J. Thrombolysis in acute myocardial infarction: analysis of studies comparing accelerated t-PA and streptokinase. J Accid Emerg Med 16, 407-411 (1999).
162 Suchkova, V. N., Baggs, R. B. & Francis, C. W. Effect of 40-kHz ultrasound on acute thrombotic ischemia in a rabbit femoral artery thrombosis model: enhancement of thrombolysis and improvement in capillary muscle perfusion. Circulation 101, 2296-2301 (2000).
163 Lew, A. S., Laramee, P., Cercek, B., Shah, P. K. & Ganz, W. The hypotensive effect of intravenous streptokinase in patients with acute myocardial infarction. Circulation 72, 1321-1326 (1985).
164 Tatu-Chitoiu, G. et al. Streptokinase-induced hypotension has no detrimental effect on patients with thrombolytic treatment for acute myocardial infarction. A substudy of the Romanian Study for Accelerated Streptokinase in Acute Myocardial Infarction (ASK-ROMANIA). Rom J Intern Med 42, 557-573 (2004).
165 GmbH, K. P. Streptokinase Karma, <https://www.streptokinase.com> (
166 Chohan, I. S., Singh, I., Vermylen, J. & Verstraete, M. Effect of furosemide on plasma fibrinolytic activity and urokinase excretion. Exp Hematol 5, 153-157 (1977).
167 Federici, A. B., Berkowitz, S. D., Zimmerman, T. S. & Mannucci, P. M. Proteolysis of von Willebrand factor after thrombolytic therapy in patients with acute myocardial infarction. Blood 79, 38-44 (1992).
168 Idell, S. Coagulation, fibrinolysis, and fibrin deposition in acute lung injury. Critical care medicine 31, S213-220 (2003). https://doi.org:10.1097/01.CCM.0000057846.21303.AB
169 Koh, S. C., Cheong, Y. C., Arulkumaran, S. & Ratnam, S. S. Coagulation activation, fibrinolysis and inhibitors in neonates. Ann Acad Med Singapore 26, 767-771 (1997).
170 Sane, D. C., Pizzo, S. V. & Greenberg, C. S. Elevated urokinase-type plasminogen activator level and bleeding in amyloidosis: case report and literature review. Am J Hematol 31, 53-57 (1989).
171 Akassoglou, K., Kombrinck, K. W., Degen, J. L. & Strickland, S. Tissue plasminogen activator-mediated fibrinolysis protects against axonal degeneration and demyelination after sciatic nerve injury. J Cell Biol 149, 1157-1166 (2000).
172 Kohler, H. P. & Grant, P. J. Plasminogen-activator inhibitor type 1 and coronary artery disease. N Engl J Med 342, 1792-1801 (2000).
173 Kranenburg, O. et al. Tissue-type plasminogen activator is a multiligand cross-beta structure receptor. Curr Biol 12, 1833-1839 (2002).
174 Zlokovic, B. V. et al. Expression of tissue plasminogen activator in cerebral capillaries: possible fibrinolytic function of the blood-brain barrier. Neurosurgery 37, 955-961 (1995).
175 Escolar, E. et al. The Effect of an EDTA-based Chelation Regimen on Patients With Diabetes Mellitus and Prior Myocardial Infarction in the Trial to Assess Chelation Therapy (TACT). Circulation. Cardiovascular quality and outcomes (2013). https://doi.org:10.1161/CIRCOUTCOMES.113.000663
176 Lamas, D. G. Intravenous Disodium Edetate (“chelation”), <http://chelation.me/category/videos/> (2019).
177 Kondo, H., Kobayashi, E., Itani, T., Tatsumi, N. & Tsuda, I. Hematology tests of blood anticoagulated with magnesium sulphate. Southeast Asian J Trop Med Public Health 33 Suppl 2, 6-9 (2002).
178 Gritters, M. et al. Citrate anticoagulation abolishes degranulation of polymorphonuclear cells and platelets and reduces oxidative stress during haemodialysis. Nephrology, dialysis, transplantation : official publication of the European Dialysis and Transplant Association – European Renal Association 21, 153-159 (2006). https://doi.org:10.1093/ndt/gfi069
179 Kario, K., McEwen, B. S. & Pickering, T. G. Disasters and the heart: a review of the effects of earthquake-induced stress on cardiovascular disease. Hypertens Res 26, 355-367 (2003).
180 Coleman, L. S. Four Forgotten Giants of Anesthesia History. Journal of Anesthesia and Surgery 3, 1-17 (2015). <http://www.ommegaonline.org/article-details/Four-Forgotten-Giants-of-Anesthesia-History/468>.
181 Mattick, J. S. Challenging the dogma: the hidden layer of non-protein-coding RNAs in complex organisms. Bioessays 25, 930-939 (2003).
182 Mattick, J. S. The hidden genetic program of complex organisms. Sci Am 291, 60-67 (2004).
183 Mattick, J. S. The regulatory architecture of the human genome. Asia Pac J Clin Nutr 13, S14 (2004).
184 Gleick, J. Chaos: Making a New Science. (1988).
185 Havlin, S. et al. Fractals in biology and medicine. Chaos, solitons, and fractals 6, 171-201 (1995).
186 Mandelbrot, B. B. The fractal geometry of nature. Updated and augm. edn, (W.H. Freeman, 1983).
ABOUT THE AUTHOR
 Lewis Coleman, MD, FAIS is a board-certified anesthesiologist who completed his BS degree in biology at Ohio State University, earned his MD degree from New York Medical College, and completed his surgical internship and anesthesiology residency at UCLA, followed by 40 years in private practice. Coleman’s basic sciences instruction at NYMC miraculously coincided with the two-year sojourn of Dr. Johannes Rhodin, a famous Swedish pioneer of electron microscopy who was retained by the school to upgrade its curriculum. Dr. Rhodin was an expert on the stress theory of Hans Selye. His stress theory lectures devastated the dogma of classical physiology and convinced Coleman that stress theory represented the future of medicine. Many years later, these lectures miraculously enabled Coleman to identify Selye’s long-sought stress mechanism. Thus identified, the stress mechanism enables Selye’s “Unified Theory of Medicine” that promises a new era of health, longevity, and freedom from the eternal curse of disease. Its implications exceed the bounds of medicine and confer a “unified theory of biology” that explains embryology, extinction, evolution, ethology, intelligence, anatomy, taxonomy, the Cambrian explosion, and dinosaurs, and resolves the disparities of Darwin, Lamarck, Baldwin, and saltation. Its distant implications reside in the realm of science fiction. His website http://www.stressmechanism.com is dedicated to stress theory and offers relevant materials free of charge. His book, 50 Years Lost in Medical Advance: The Discovery of Hans Selye’s Stress Mechanism, is available on Amazon.
Lewis Coleman, MD, FAIS is a board-certified anesthesiologist who completed his BS degree in biology at Ohio State University, earned his MD degree from New York Medical College, and completed his surgical internship and anesthesiology residency at UCLA, followed by 40 years in private practice. Coleman’s basic sciences instruction at NYMC miraculously coincided with the two-year sojourn of Dr. Johannes Rhodin, a famous Swedish pioneer of electron microscopy who was retained by the school to upgrade its curriculum. Dr. Rhodin was an expert on the stress theory of Hans Selye. His stress theory lectures devastated the dogma of classical physiology and convinced Coleman that stress theory represented the future of medicine. Many years later, these lectures miraculously enabled Coleman to identify Selye’s long-sought stress mechanism. Thus identified, the stress mechanism enables Selye’s “Unified Theory of Medicine” that promises a new era of health, longevity, and freedom from the eternal curse of disease. Its implications exceed the bounds of medicine and confer a “unified theory of biology” that explains embryology, extinction, evolution, ethology, intelligence, anatomy, taxonomy, the Cambrian explosion, and dinosaurs, and resolves the disparities of Darwin, Lamarck, Baldwin, and saltation. Its distant implications reside in the realm of science fiction. His website http://www.stressmechanism.com is dedicated to stress theory and offers relevant materials free of charge. His book, 50 Years Lost in Medical Advance: The Discovery of Hans Selye’s Stress Mechanism, is available on Amazon.
Combat Stress Magazine
Combat Stress magazine is written with our military Service Members, Veterans, first responders, and their families in mind. We want all of our members and guests to find contentment in their lives by learning about stress management and finding what works best for each of them. Stress is unavoidable and comes in many shapes and sizes. It can even be considered a part of who we are. Being in a state of peaceful happiness may seem like a lofty goal but harnessing your stress in a positive way makes it obtainable. Serving in the military or being a police officer, firefighter or paramedic brings unique challenges and some extraordinarily bad days. The American Institute of Stress is dedicated to helping you, our Heroes and their families, cope with and heal your mind and body from the stress associated with your careers and sacrifices.
Leave A Comment
You must be logged in to post a comment.