To Conserve the Fighting Strength. Sex Modifying Medications and Psychiatric Standards of Fitness in the U.S. Military: A Repeat of McNamara’s 100,000
By MAJ (RET) C. Alan Hopewell, PhD, MP, ABPP, BSM
and CPT Robert Klein, PhD, US Army
*This is an article from the Fall 2023 issue of Combat Stress
The History of Cross Sex Military Service
The United States military has a long history of female service personnel masquerading as males, dating back at least to the War Between the States. Initially, all such Service Members were women who disguised themselves as men in order to serve in military roles, presumably for various personal advantageous reasons. Two such famous women were Jennie Irene Hodgers, who impersonated a male Soldier in the War Between the States, and Cathay Williams, a female and former slave who disguised herself in order to serve as a Buffalo Soldier during Western service in the Indian Wars. PVT Williams even has a plaque honoring her service in Trinidad, Colorado. Obviously, no males are known to have masqueraded as females in order to serve in the military, and none of the women who disguised themselves as men really believed that they were the opposite sex. However, in more recent years, an increasing number of both males and females with what is now diagnosed as “gender dysphoria”16 have served or have sought to serve in the military.
Beginning on June 30, 2016, and through January 1, 2018, the cohort now known as “gender dysphoric individuals” became eligible to serve in the United States military “upon completing transition.” From January 1, 2018, to April 11, 2019, gender dysphoric individuals could enlist in the United States military under the condition of being stable for 18 months in presenting themselves in public with behaviors normally associated with the opposite sex. On June 30, 2016, Secretary of Defense Ash Carter, never having served in the Armed Forces himself, made an official announcement and published Directive-Type Memo 16-005 (DTM 16-005)8 on this issue. From January 26, 2021, onwards, there have been no restrictions on military service by gender dysphoric individuals. However, contrary to the requirement in Directive-Type Memo 16-005 (DTM 16-005) that
- … “Transgender (sic) Soldiers will be subject to the same standards as any other Soldier of the same gender (sic)”

such standards are already being routinely ignored, as these Soldiers are far from subject to the same physical training standards as are regular Soldiers61 and such Soldiers apparently also do not need to be concerned about deployment requirements which affect all other military personnel. The question is also raised if these Soldiers are also being held to the same mental and legal requirements of others in that the first Soldier processed under this directive, U.S. Army MAJ Jamie Lee Henry, has already been arrested for conspiracy and wrongful disclosure of individually identifiable health information,45 raising the question of if sexual confusion can ever be divorced from questions of psychiatric dysfunction, especially in cases such as Henry and Bradley Manning. A previous well known case involved sexually confused Soldier Bradley Manning, arrested and convicted of in July 2013 of violations of the Espionage Act and other offenses.39
Advocates of sexually confused individuals serving actively in the Armed Forces argue that there should be no concerns about such service and that such Soldiers, Sailors, or Airmen present no problems or burdens to service, being as “fit” as others for military service (Caputo;57 Elders and Satcher,18 and Klimas37). However, none of these individuals ever served in combat, never worked with Soldiers in Basic or Advanced Individual Training (AIT) as well as both in deployed theaters and in garrison (as have both authors,) and never served on a sexual surgery team at a major U. S. medical school as did the senior author. None of them ever managed the medication treatment of Soldiers in the most hostile combat environments imaginable, as did the senior author. Significant problems also occur on submarines or on naval surface ships, especially with those without a fully qualified Medical Officer on board, and can also occur during strenuous exercises prior to actual deployment such as Joint Readiness Training Center/ National Training Center (JRTC/NTC) operations, as have been experienced by the authors. Even a cursory glance at the medical and psychiatric care required by “gender dysphoric” individuals provide compelling proof that an increased burden of medical and psychiatric care is engendered under such circumstances and that this may be particularly problematic in combat or in challenging deployment conditions. Many such individuals may be ineligible for initial induction under normal circumstances due to their co-morbid psychiatric disorders or may be particularly prone to later Chapter or Medical Board separations.
The “opinions” of bureaucrats, ideologs, or “experts” do not count, unless backed up by solid experience, as was shown in the devastating debacle that was known as Project 100,000 or “McNamara’s 100,000.”29 This is especially true of “opinions” which are based upon “feelings” rather than empirical research, preferably that which would meet Daubert standards14 as well as evidence-based research requirements. For example, during the Vietnam War Robert McNamara and Lyndon Johnson had great “feelings” and “compassion” for those with intellectual disabilities, but the military experience of seasoned officers and the eventual solid evidence-based research proved how terribly mistaken they were about Project 100,000. The correct “solution” to the “problems” identified by McNamara and Johnson would have been never to have inducted this cohort into the Armed Forces to begin with.29
The induction of large numbers of previously unfit individuals into the Armed Forces unfortunately has a catastrophic historic precedent and occurred during the Vietnam War under a program known as “Project 100,000 or McNamara’s 100,000.”29 Project 100,000 was initiated by Defense Secretary Robert McNamara in October of 1966 to meet the escalating manpower requirements of the American government’s involvement in the Vietnam War (the “problem”) and to provide a “compassionate” way to improve the sociological, mental, and financial plight of some of America’s poor and uneducated (the “solution”). In one sense this was no different from a number of seemingly “progressive” ideas that people as well as plants can be improved by environmental engineering which will eventually overcome genetic and Mendelian parameters of biological functioning, the latter idea about plants being espoused by the Soviet agriculturist Trofim Denissovich Lysenko (Kean;36 Oury48). Eventual research showed that inductees of Project 100,000 died at triple the rate of other Americans serving in Vietnam and that following their service, this cohort of inductees had lower incomes and higher rates of divorce than their non-Veteran counterparts.29 The project was ended as a complete and abject failure on the part of both McNamara and Johnson in December of 1971, although the effects of this disaster dragged on for years, as the senior author was still dealing with some of the residuals of this program as late as 1978 at Fort Jackson, South Carolina.
Robert McNamara and the bureaucrats who supported “McNamara’s 100,000” held such ideas for lofty but naïve reasons, and the program was never grounded in reality. The opinions of ideologues such as Caputo, Elders, Satcher, and Klimas similarly really count for nothing except childlike reflexive support of erroneous ideological ideas. Like Robert McNamara, who framed his program in terms of “compassion,” and thought that the “technology” of the times would result in these men being fully functioning members of the Armed Forces, current apologists seem to believe that medications and surgery – today’s most advanced “technology” – will have similar results for sexually confused Servicemen and women. Robert McNamara and Lyndon Johnson ignored repeated advice and concerns from real Soldiers who served in real conditions in the Armed Forces,29 and today’s advocates seem to be once again repeating the mistake of relying on ideology rather than realism. Such problems and patterns of poor decision making based on ideology rather than science and evidence-based practice unfortunately seems to occur in cycles.
One such cycle was that of Trofim Denissovich Lysenko who was a fraud Soviet “agricultural scientist.” Like current clinicians who ignore the genetic basis of sex and sexuality, Lysenko claimed that Mendelian genetic science and the chromosomal basis of biological development were all irrelevant to the development of putative resilient plant species. Since Soviet ideology asserts that environmental factors are paramount in human development and that differences between people or plants are simply “social constructs,” organisms can “develop” into different physical and metabolic forms based upon environmental exposure, introduced chemical agents, and forced physical alterations of the biological system (in Lysenko’s case plants). Based on Lysenko’s theories in the late 1920s and early 1930s, Joseph Stalin undertook a “modernization of Soviet agriculture” by forcing these theories onto Soviet science and agricultural practice. This simply resulted in widespread famines that killed more than seven million people. It should be noted that the Soviet Union’s allies also adopted Lysenko’s methods with even worse results. China’s population suffered even more as the number of victims is estimated at more than 30 million (Kean;36 Oury48). Similar to medical personnel who are now lionized as “innovators” in sexual surgery, Lysenko became a real hero in the Soviet Union and the inventor of “miraculous techniques” to transform biological organisms even while people were starving to death. In 1938, the Council of People’s Commissars of the USSR fast tracked him to the head of the Lenin Academy of Agricultural Sciences. It should be noted in passing that as Lysenko ascended the ranks of power, he attacked scientists who defended genetic theories and destroyed their careers in similar ways to those currently being attacked for questioning the basics of “affirming care” for sexually confused individuals, and in many of the same ways in which line Officers during the Vietnam era were attacked and their careers put in jeopardy for questioning the all too predictable outcomes of “McNamara’s 100,000” (Kean;36 Oury48).
“Transexualism” as a Pseudo Disorder
Settled science has documented that a person’s sex is comprised of chromosomal composition, with approximately 37 trillion of these cells being the “blueprint instructions” for each and every cell in the human body.6 It is not possible to change these or to change even a single cell in ANY human body from “male to female” or from “female to male.” Ideologues often like to quote extremely rare occurrences of intersex births or disorders such as Klinefelter’s syndrome (YXX) which, of course, have nothing to do with the issue at hand. In addition, even these conditions cannot be “changed” genetically.49 Therefore, it is not possible for any human to “change their sex” or become “transexual” or “transgender,” (“gender” being a literary rather than a scientific sexual term,) but they are only able to modify physical function and cosmetic appearance by means of pharmacology, clothing, cosmetics, surgery, and / or learned behavior. Therefore, the very terms “transexual” as well as “transgender” are inaccurate, misleading, and nonscientific, and will not be used in this paper due to the inaccuracy and impossibility of these terms.
Also, one occasionally hears the statement that “so and so was born a male in a female body,” or with a “male brain in a female body,” or vice versa, but again, this is not possible. The Chairman of the Diagnostic and Statistical Manual (DSM) committee which included the term “gender dysphoria” is Kenneth Zucker. Zucker has stated that this is a diagnosis with absolutely no objective markers and one which anyone, at any time, under any circumstances, can simply claim. He also points out two advantages of making up a diagnosis of “gender dysphoria.” The first advantage in constructing such a diagnosis is that a finding of Delusional Disorder could therefore be avoided, and sexually confused individuals would not be classified as psychotic or delusional. The second advantage is that insurance benefits, much like the medical benefits now offered by the Armed Force and the Veterans Administration, could also be provided.73 However, the advocates of including a diagnosis of a gender disorder in the DSM possibly failed to anticipate the irony that anyone claiming this disorder would now be officially meeting the criteria for a formal mental illness, whether the illness is called a “disorder” or a “dysphoria.”
Such issues also raise the question that at least some “gender disordered” individuals may attempt to be recruited into military service not from a sense of any national duty or commitment, but because they see the military as a large “insurance/ health care agency” which can provide them with this type of care. This, once again, mimics the problems found with the “McNamara’s 100,000” project, in that one half of the reasoning for inducting substandard Soldiers was to take care of them in terms of a sociological agenda. Research conducted on retention factors for military personnel and health care issues have long and firmly established that such motivations are strong predictors that such Soldiers will fail to be retained in the military and that they are poor induction prospects (Gregory;29 Hopewell and Ozburn32).
Dr. Paul R. McHugh, the former psychiatrist-in-chief for Johns Hopkins Hospital, where John Money’s failed sex treatment clinic was closed for malpractice after the suicides of some of his patients, concurs with the DSM that gender dysphoria is a “mental disorder” that merits psychiatric treatment, that sex change is “biologically impossible,” and that people who promote sexual reassignment surgery are collaborating with and promoting a mental disorder. Dr. McHugh, one of the foremost sex experts in the entire world, has indicated that “sex change” is biologically impossible and that there is no scientific evidence that any person is “born into the wrong sexual body.” The evidence does demonstrate, however, that people who undergo sex-reassignment surgery do not change from men to women or vice versa. Rather, they merely become feminized men or masculinized women.41 The main difference is that instead of simply wearing transvestite clothing and adopting behaviors of the opposite sex, they additionally often undergo drug induced and surgical changes.
Co-Morbidity of Mental Disorders Among This Population
ALL sexually confused individuals are therefore mentally ill by their own definition, and as many as 80 percent display a large number of co-morbid disorders, making correct diagnoses and psychotherapy essential.43 The most frequent of such co-morbid disorders include those of substance abuse, schizophrenia, bipolar disorder, depression, anxiety disorders, personality disorders, autism, attention deficit disorders, self-harming behaviors, and those susceptible to hysterical epidemics (borderline personalities and young teenage girls, especially with autism, etc.25 Since many such disorders will mandate either limited military service or chapter/ medical separation from service, the recruitment of such inductees is anticipated to create an increasing burden upon military health care as well as upon administrative separations.2
Some of these incapacitating conditions or disorders requiring separation include:
- Current or history of disorders with psychotic features such as schizophrenia, paranoid disorder, and other unspecified psychoses, such as delusions of being the other sex.
- Current mood disorders including, but not limited to, major depression, bipolar, affective psychoses, and depressive not otherwise specified.
- History of mood disorders requiring outpatient care for longer than 6 months by a physician or other mental health professional, or inpatient treatment in a hospital or residential facility.
- History of symptoms consistent with a mood disorder of a repeated nature that impairs school, social, or work efficiency.
- Current or history of adjustment disorders within the previous 3 months.
- Current or history of misconduct or behavior disorders.
- Recurrent encounters with law enforcement agencies, antisocial attitudes or behaviors that are tangible evidence of impaired capacity to adapt to military service (demonstrated by some “gender nonconforming” individuals).
- Current or history of personality disorders.
- History (demonstrated by repeated inability to maintain reasonable adjustment in school, with employers or fellow workers, or other social groups), interview, or psychological testing revealing that the degree of immaturity, instability, personality inadequacy, impulsiveness, or dependency will likely interfere with adjustment in the Armed Forces is disqualifying (almost a sine qua non of many sexually confused individuals).
- Current or history of other behavior disorders including, but not limited to conditions such as a history of suicidal behavior or history of self-mutilation.
- Current or history of anxiety disorders (anxiety or panic), agoraphobia, social phobia, simple phobias, obsessive-compulsive, other acute reactions to stress, and posttraumatic stress disorder.
- Current or history of dissociative disorders, including, but not limited to hysteria, depersonalization, and others (related disorders).
- Current or history of somatoform disorders (“gender dysphoria,”?) including, but not limited to hypochondriasis or chronic pain disorder.
- Current or history of psychosexual conditions, including, but not limited to transsexualism, exhibitionism, transvestism, voyeurism, and other paraphilias.
- Current or history of alcohol dependence, drug dependence, alcohol abuse, or other drug abuse.
- Current or history of other mental disorders that in the opinion of the civilian or military provider will interfere with or prevent satisfactory performance of military duty.
Such conditions are even more problematic during conditions of deployment, especially in hostile combat environments in which medical care may be limited.62 United States European Command Instruction regulations require, for example, that:
- Personnel who require medication(s) will travel with up to a 180-day supply of their maintenance medications (see paragraph 1.h.(2) below for controlled medication requirements).
- Controlled Medications. All FDA controlled substances (Schedule CII-CV) are limited to a maximum of a 90-day supply in-theater, with only 30 days’ supply allowed on the person. All controlled substances need to be secured (i.e., to prevent diversion). Controlled substances must be monitored using a validated quality assurance program.
- Prior to deploying, individuals need to arrange to obtain a sufficient supply to cover the remainder of the deployment.
Individuals also need to be aware that certain countries (i.e., Germany) prohibit the mailing of prescription medications. Note also that many Soldiers and military personnel who are deployed to other areas may need first to transit through Germany on their way to other deployments or may, by necessity, need to be deployed back or evacuated to/through Germany such as those evacuated to the Traumatic Brain Injury Clinic founded by the senior author at Landstuhl Army Medical Center, so these or similar regulations may well apply regardless of the Soldier’s deployment status.31 Other conditions noted by USEUCOM include issues of:
- Border Clearance. Medical conditions must meet border clearance criteria of the countries in which the individual will be deployed (note that some countries may refuse admission to certain sexual conditions and/ or medications).
- Ability to Function During Flare-Up. Medical condition must not reach severity which completely incapacitates the individual.
- Alert and Oriented. The individual must be alert and able to perform sensitive tasks with appropriate judgement when required (i.e. medications causing drowsiness must clear the body quickly).
- Functional in Austerity. Individuals must be of sufficient fitness to successfully function and conduct the mission in the extremes of environmental conditions while wearing appropriate protective gear.
- Low Risk to Command. The medical condition must not place coworkers at safety risk or at risk for mission failure.
- Severity of medical condition. Conditions must be of sufficient simplicity to be managed by a general medical officer in facilities with limited equipment (emphasis added – a direct violation of the guidelines of the World Professional Organization for Transgender Health (WPATH) which argues exactly the opposite.24
The use of psychoactive medications also poses additional risk in the deployment environment, such as risk for heat injury, serotonin syndrome, lapses in judgment and alertness, etc. These medications are commonly used to treat depression, insomnia, drowsiness, concentration and alertness problems, mood disorders, anxiety, chronic pain, migraine headaches, seizures, etc., many of the exact co- morbid disorders from which many sexually confused people suffer. The following concerns will be scrutinized closely when considering waivers for psychoactive medications:
- Behavioral effects. Psychoactive medications affect alertness, sleep cycle, and judgment; all effects can be magnified when multiple medications are combined.
- Suicide risk. Psychoactive medications pose additional risk for suicide based on the physiologic effects of the medications, and in their normal use by patients at higher risk for suicide.
- Polypharmacy concerns. Medications prescribed to counter-act the side effects of other medications are problematic, due to compounding of side effects (i.e., treating awakeness (sic) and alertness, while also addressing insomnia) and contribution to polypharmacy.
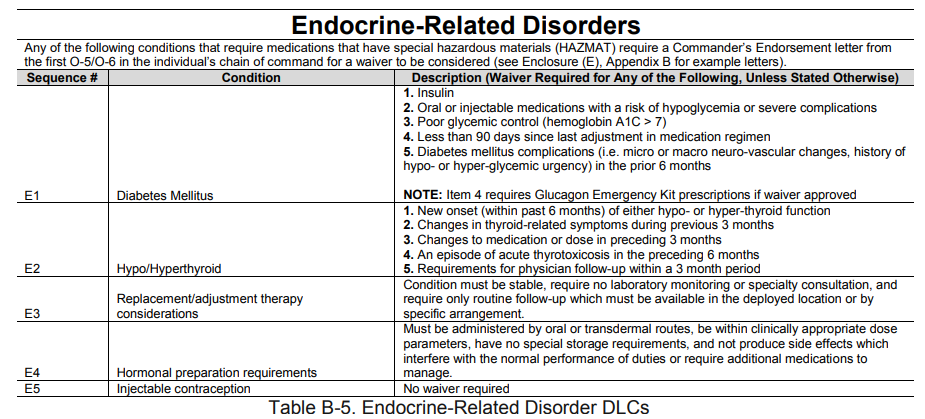
Some of the conditions related to endocrine circumstances are summarized in Table B-5, and indicate the difficulty of managing some of these conditions under circumstances of deployment by a general medical officer in facilities with limited equipment, or in many circumstances by a nurse or a Physician’s Assistant ( PA) who may be supervised by a Medical Officer who is not even in the same facility, as experienced directly by the authors during combat conditions, or as is frequently the case in some Naval convoys. As Cone and Oliverson have testified,11 the long-term management of these agents is extremely problematic and even gender dysphoric individuals enrolled in specialized gender clinics frequently have trouble receiving adequate care as so few specialists exist or are willing to assume the liability for such treatment. This cannot be considered adequate treatment, such as the management of hypothyroidism where an endocrinologist “gets the dose of Synthroid correct” and then pushes the management down to a Family Practitioner or a master’s degree clinician who can simply dispense the medication endlessly.
The psychiatric disorders list is extensive, and will not be repeated here, but almost any of these disorders could be manifested by sexually confused individuals with these co-morbid disorders. These sexual disorders are also mentioned in Table B-18, with the risks of suicide, psychiatric disorders, and psychiatric burdens clearly identified:
Note that “the gaining unit [must possess] personnel who know the normal baseline of the transitioned person, and can recognize high risk variations,” and that “leadership determination of risk, especially for high-risk positions” is required. Would anyone really think that such resources are readily available in most deployed commands? Perhaps only naïve individuals who never even served in the Armed Forces, such as Carter, Elders, Klimas, and Satcher, or those not involved in warfare operations such as Caputo.57 To further “pound in” how completely unfit even the Army considers these recruits to be, they are now exempted from any type of Physical Fitness testing as well.61
A5.5 Approved Exemptions
A5.5.1 The unit commander, or equivalent, will sign a memo authorizing the exemption. ![]()
A5.5.2. Unit Fitness Program Managers (UFPM) will document the exemption in myFitness, using the commander’s composite exemption.61
Who would think, therefore, that a Service Member who is unfit to deploy and unfit even to meet basic physical training standard while sitting behind a desk in a Continental United States (CONUS) garrison will be of much use to the Armed Forces, any more than the vast majority of McNamara’s 100,000 inductees were? Note also that every geographic Combatant Command (COCOM) has rules for medical fitness which might vary; Bahrain’s being very strict, and some geographic areas do not permit entry to persons with what are classified in those cultures as sexual disorders.
Suicidality and Co-Morbid Mental Disorders
It has now been documented in a large number of studies in several different countries (England, Sweden, Norway, Finland, Holland, and the U.S, at Case Western Reserve University) that the majority of such sexually confused individuals may present with serious psychiatric disorders, to include autism spectrum disorder, borderline personality disorder, depression, and at times delusional disorders. For example, autistics necessitating mental health treatment for their autism spectrum disorders are now seven times more likely to identify as sexually confused than the general population (Vrangalova68 and Warrier70). A study by Meybodi43 has found the rate of co-morbid personality disorders among sexually confused individuals to be as high as 81.4 percent. Therefore, even a cursory glance at the medical and psychiatric care required by gender dysphoric individuals provides compelling proof that an increased burden of medical and psychiatric care is engendered under such circumstances, and that this may be particularly problematic in combat or challenging deployment conditions.
The prevalence of autism or mild autistic traits, for example, has been shown to be very common among people with gender dysphoria relative to the general population. Even less frequent diagnoses, such as bipolar or personality disorders, are relatively common among people with gender dysphoria.25 Regarding self-harming behaviors, including attempts at suicide, the incidence is also documented to be increased among people with gender dysphoria, especially among young people ages 18 to 24 (a prime age for potential military induction). Among this cohort, depressive and anxiety disorders are also commonplace and again, exactly within the age range which would be “prime induction ages” for most military recruits; Swedish studies determined that 18.2 percent to 25 percent of those patients identifying as gender dysphoric suffered from major depression, 20.9 percent to 28.5 percent from anxiety disorders, 3.6 percent to 4 percent from personality disorders, 14.7 percent to 16.3 percent from autism spectrum disorders, 13.5 percent to 18.4 percent from ADHD etc., and 4.9 percent to 13.7 percent from self-harm.25 All of these disorders, in addition, may result in either increased burdens for medical care during military service, limited duty requirements, and/or necessitate outright separation from service on psychiatric grounds.2 
In addition, settled science has shown that sexually confused individuals demonstrate a significant increase in suicides over the general population.25 This report documented a 4.9 and 13.7 times increase in the risk of suicide, respectively, as compared to the general population. Research by agencies supportive of gender confusion issues have themselves found that data indicate that 82 percent of transgender individuals have considered killing themselves and 40 percent have attempted suicide, with suicidality highest among transgender youth, the age range of many potential recruits.3 A 1984 study of transgender individuals requesting sex-reassignment surgery showed even higher suicide attempt rates between 19 percent and 25 percent.22 Finally, a large sample of 40,000 primarily U.S. volunteers completing an internet survey in 2000 found transgender persons to report higher rates of suicide attempts than any group except lesbians.41 This is all confirmed by the most recent comprehensive study to date, a study undertaken in Denmark.
A report from the American Foundation for Suicide Prevention and the Williams Institute,30 a think tank for LGBT issues at the UCLA School of Law, summarized findings about suicide attempts among sexually confused adults from a large national sample of more than 6,000 individuals. This constitutes the largest study of such adults to date.
Summarizing the major findings of this study, the authors write:
“The prevalence of suicide attempts among respondents to the National Transgender Discrimination Survey (NTDS), conducted by the National Gay and Lesbian Task Force and National Center for Transgender Equality, is 41 percent, which vastly exceeds the 4.6 percent of the overall U.S. population who report a lifetime of suicide attempts, and is also higher than the 10 to 20 percent of lesbian, gay and bisexual adults who report ever attempting suicide.”
At the same time, people with gender dysphoria who committed suicide also had very high rates of serious psychiatric diagnoses, such as harmful use or addiction to various substances, schizophrenia or personality disorders (such as borderline personality disorder). As a result, what is clearly known is that suicide risk among people with gender dysphoria and other co-occurring psychiatric diagnoses is much more pronounced than within the general population. With the concern of the military for increased suicides over the past decade or so, this is certainly a very prominent concern.12 The Armed Forces have a high enough suicide rate; why make attempts to recruit a cohort where the rate is catastrophic? Additional concerns are presented when such individuals must be seen by mental health personnel and at times subsequently be medically evacuated out of the wartime theater, at times from combat or hostile service areas. The 785th Combat Stress Control (CSC) Company, based out of Fort Snelling, Minnesota, for example, during its second tour of Iraq, had the most mental health contacts of any CSC in Operation Iraqi Freedom (OIF) – well over 40,000 contacts. Although being successful at retaining more than 98 percent of all CSC patients in theater, the remaining 2 percent who had to be medically evacuated to CONUS comprised a considerable number and created substantial psychiatric demands on medical staff. In addition, at Fort Hood alone, these evacuations accounted for approximately 2 to 4 returning Solders every day, resulting in increased psychiatric burdens on the receiving units and hospitals.12 At the time, Carl Darnall Army Medical Center, although an Echelon IV Army Medical Center, could not meet all of the psychiatric needs of these returning Soldiers, and was forced to transfer Soldiers needing ongoing care to civilian facilities as far away as Dallas and San Antonio. They were also reduced to relying on psychological screening “tests” that were downloaded from the internet, as mental health services could not meet the pressing needs.58 Combine this with the even greater naval burdens of evacuating suicidal Sailors from a naval ship or submarine and the ongoing care of such personnel under even normal circumstances. This became astoundingly burdensome. None of such mental health treatment programs could be reasonably expected to provide the higher echelon care needed by gender dysphoric individuals on dangerous medication regimens, or even the complicated psychiatric symptoms constellations presented by such patients.
The second reason for increased burdens includes the nature and effects of many of the drugs taken for gender dysphoria, as well as the possible long-term effects on a Soldier’s mental as well as physical wellbeing. This latter issue has, to the best of the knowledge of the authors, never really been addressed in the literature and will therefore be the focus of this paper.
Puberty Blockers and Cross Sex Hormones
Medications taken by gender dysphoric individuals in an attempt to “become” the opposite sex generally include two different classes: the so called “puberty blockers” and cross sex hormones. The medications most commonly used to suppress puberty are known as gonadotropin-releasing hormone (GnRH) analogues. “Puberty blockers,” also known as gonadotropin-releasing hormone (GnRH) analogues, were introduced for medical use in the 1980s63 and were originally developed to supersede other therapies in the treatment of prostate cancer. While it is uncertain how many military recruits would enter service on such medications, a large number may have taken them in the past and may well still be experiencing the lingering effects of such agents, since the effects are not reversible, as claimed by some ideologues.
GnRH is a naturally occurring hormone in humans responsible for the release of follicle-stimulating hormone (FSH) and luteinizing hormone (LH) from the pituitary gland. Through this mechanism, the body produces its gonadal estrogen and testosterone. GnRH agonists bind to the GnRH receptor and activate it, causing it to be continuously stimulated. This causes an initial increase of LH and FSH. Then over the course of several weeks this causes the pituitary gland to become desensitized, pausing the natural sex hormone production. Although proponents of using these agents claim that the effects are “reversible,” this has been shown NOT to be the case and in fact long term use can cause permanent suppression of the hypothalamic/ pituitary/ gonadal axis.47 In addition, many of these circuits overlap, such as with the hypothalamic/ pituitary/ adrenal axis, which is known to be disrupted in cases of post-traumatic stress disorder.47 The gonads and the adrenal glands are involved in two separate, but interrelated pathways (or “axes”) of hormone signaling: the hypothalamic-pituitary-gonadal (HPG) axis and the hypothalamic-pituitary-adrenal (HPA) axis. Therefore, the use of such drugs prior to military service may actually increase the vulnerability of such individuals to later dysfunction in brain circuits, especially if they are exposed later to severe stress or develop PTSD.
Short-term side effects of puberty blockers include headaches, fatigue, insomnia, muscle aches and changes in breast tissue, mood, and weight. After exhaustive study, these medications have been banned in England due to the serious side effects experienced by children given these agents (Barnes;5 Transgender Trend65). Long term effects may be even more serious, and more than 10,000 adverse event reports filed with the FDA reflect the experiences of women who have taken Lupron. Lupron (Leuprolide) is one of the gonadotropin-releasing hormone (GnRH) analogues which was originally developed as an anti-neoplastic agent to combat prostate cancer and is one of the most dangerous drugs on the market due to its low therapeutic index.29 Like other gonadotropin-releasing hormones, the drug interacts with DNA or its precursors, inhibiting the synthesis of new genetic material or by causing irreversible damage to the DNA itself. By disrupting cell cycles and preventing the body from producing normal sex hormones, the expected development of puberty is blocked, and both the brain and physical characteristics of the body known as the secondary sex characteristics are disrupted. Reports of adverse effects describe everything from brittle bones to faulty joints and include depression, anxiety, suicidal urges, and seizures – all of these potentially service-disqualifying. Drugs used to halt puberty in children are also known to cause lasting health problems in adults.34 Among men who take Lupron, its label warns of increased risk of heart attacks, strokes and sudden death. Adverse effects on bone mineralization, loss of bone density, osteopenia, chronic pain, and compromised fertility are also now well-known adverse effects of pubertal suppression secondary to GnRH agonists.71
Research on the long-term effects on brain development, cognitive function, fertility, and sexual function is limited, but researchers suspect that a number of long-term problems may eventually be better documented (Terhune, Respaut, and Conlin63 and Rosenthal55). Consistent with this, a study conducted by Chen and other researchers9 suggested that “pubertal suppression may prevent key aspects of development during a sensitive period of brain organization,” adding that “we need high-quality research to understand the impacts of this treatment – impacts which may be positive in some ways and potentially negative in others.” In 2016, the FDA even ordered drugmakers to add warning labels to puberty blocker drugs stating: “Psychiatric events have been reported in patients,” including symptoms “such as crying, irritability, impatience, anger and aggression.” In 2022, the FDA also reported an increased number of cases of idiopathic intracranial hypertension and pseudotumor cerebri in patients taking puberty blockers.53
Hormones responsible for sexual differentiation are generally thought to exert on the developing fetus either organizational effects — which produce permanent changes in the wiring and sensitivity of the brain, and thus are considered largely irreversible — or activating effects which occur later in an individual’s life (at puberty and into adulthood). Organizational hormones may prime the fetal systems (including the brain) structurally and set the stage for sensitivity to hormones presenting at puberty and beyond. The hormone will then “activate” systems which were “organized” prenatally. It must be noted that the primary goal of puberty blockers is to disrupt the normal development of the brain and the resulting instructions to the body for psychosexual development. However, considerable evidence exists that there are specific “windows” for critical brain development in children, and if this development does not take place at the appropriate time, permanent and irreversible damage or lack of proper development may occur, such as in the case of feral children and poverty of language development (Birdsong,7 Curtiss,13 Mihai44).
Similar issues may also occur in youngsters given chronic gonadotropin-releasing hormone agonist (GnRHa) agents in that there is now documented evidence of disruption of long-term memory in sheep who have had their brain function disrupted in this manner.33 Hougha et al. note that these adverse results suggests that the time at which puberty normally occurs may represent a critical period of hippocampal plasticity, and that perturbing normal hippocampal formation in this peripubertal period may also have long lasting effects on other brain areas and aspects of cognitive function. The effects do NOT appear to be reversible and would be of even increasing concern in a male who had taken puberty blockers prior to enlistment, who had subtle effects on memory function, and then had possibly increased cognitive decline as they continued to deliberately manipulate their hormone levels as an adult.
Goodman and Gilman’s authoritative text on therapeutics notes that “few categories in medicine in common use have a narrower therapeutic index and a greater potential for causing harmful side effects than do the antineoplastic drugs – the puberty blockers”28 (emphasis added pg. 1381.) Agents in this category typically used with sexually confused patients include the adrenocortical steroids, progestins, estrogens, antiestrogen, androgens, and gonadotropin-releasing hormone analogs. Note that although Soldiers might have been prescribed some agents only during puberty, such as the gonadotropin-releasing hormone analogs, the effects of these agents are now known to last over the lifespan. Recent testimony from a 45 year old individual who is well within military active or retirement age range illustrates these problems.11 During legislative testimony, Cone11 testified that he had trouble receiving adequate medical care as he aged and had increasing difficulty with the side effects of drugs on his body and his abnormal hormonal levels. Being on hormones for three decades, he is no longer able to produce his own hormones and must rely solely on hormone replacement therapy. He is now increasingly concerned, since low testosterone levels have been linked to dementia in males, but he can find no neurologist or endocrinologist outside of a “gender clinic” to treat him. Even though he was a civilian residing in CONUS with presumed access to full medical care, he explained that most physicians would refuse to attempt to treat him at this stage of his numerous medical problems and would uniformly try to refer him to “gender clinics.” When attempting to access care at such clinics, however, Cone found that such “clinics” are over-burdened and do not follow the standard of care promulgated by the World Professional Association for Transgender Health (WPATH) by almost uniformly having no specialists, such as endocrinologists, on staff. In addition, although Cone is a professional with advanced IT experience and employed in that position, even he has been unable to find a “gender clinic” which has a neurologist or endocrinologist on staff to treat him properly in his state of residence. Cone also asserts that no adequate research exists at all for people at this stage of hormone therapy and that no clinicians exist who are experts in coping with these complications. He also asserts that patients such as this will often resort to obtaining drugs and hormones illegally and without proper prescription. Entire communities exist which produce “bathtub estrogen” for use by these patients (essentially home-produced drugs). This begs the question: if a knowledgeable and medially sophisticated patient such as this, treated with the best medical care available for three decades, with adequate medical insurance, residing within CONUS and with access to all preferred medical care cannot receive adequate care at this stage in life, how can we expect to provide an adequate level of care to Soldiers who may often be deployed as well as expected to function under conditions and in locations where such care would be impossible? Note that current deployment guidelines require that medical care and medications be dispensed by “a general practitioner,” meaning that it would be against regulations to deploy Soldiers needing such specialist care to areas in which it is not available. This would also be in violation of WPATH guidelines which state that “The (doctor) is not merely a technician hired to perform a procedure; the (doctor) is part of the team of clinicians participating in a long-term treatment process.”24 This is exactly what most military treatment facilities, especially outside of CONUS, do not have and cannot offer: a “team of clinicians participating in a long-term treatment process” for a specialty as complicated as sexually confused individuals with extremely high co-morbid psychiatric disorder rates and rates of potential suicide, and taking drugs off label with long-term and unknown effects. This is hardly the case of “these patients are simply taking the equivalents of birth control pills” so casually stated and cynically dismissed by Caputo,57 a Coast Guard Officer with no combat experience.
Problems with the Anabolic-androgenic Steroids
Once a potential military recruit has ceased taking puberty blockers, however, they must continue to take “cross sex hormones” if they wish to maintain the fiction of “being the opposite sex.” These normally constitute the androgens, which are various ratios of testosterone and estrogen – the very agents that are usually banned in sports competitions and are well known to place individuals at risk for a number of health issues, to include “roid rage.” The use of testosterone agents even seems to have contributed to the very well-publicized death of a recent Navy SEAL candidate Kyle Mullen.17
Natural testosterone is a steroid — an anabolic-androgenic steroid. “Anabolic” refers to muscle building, and “androgenic” refers to increased male sex characteristics. However, when one hears the term “anabolic steroids,” they are generally referring to synthetic (made in a lab) variations of testosterone that are injected into the body. Healthcare providers use synthetic testosterone to treat and manage various medical conditions and these agents are generally safe when used medically appropriately. Synthetic testosterone is the main drug of masculinizing hormone therapy, which is a treatment used to produce the male secondary sex characteristics. Although most studies have been done with males taking testosterone, similar adverse effects may occur with females who are on these agents for long periods of time. Prolonged use of high doses of androgens (principally the 17-α alkyl-androgens) has been associated with development of hepatic adenomas, hepatocellular carcinoma, and peliosis hepatis — all potentially life-threatening complications. There have been post-marketing reports of venous thromboembolic events, including deep vein thrombosis (DVT) and pulmonary embolism (PE), in patients using testosterone products.
Testosterone, as testified by Cone47 is frequently subject to abuse by sexually disordered patients, typically at doses higher than recommended for the approved indication and in combination with other anabolic androgenic steroids. Anabolic androgenic steroid abuse can lead to serious cardiovascular and psychiatric adverse reactions. In diabetic patients, the metabolic effects of androgens may decrease blood glucose and, therefore, insulin requirements. There are also reports of hepatocellular carcinoma in patients receiving long-term therapy with androgens in high doses. Withdrawal of the drugs did not lead to regression of the tumors in all cases.
Known effects of testosterone use include, but are not limited to: increased blood pressure, increased risk of myocardial infarction, bleeding from the gums or nose, bloating or swelling of the face, arms, hands, lower legs, or feet, blurred vision, bone or muscle pain, discouragement, dizziness, eye pain, feeling sad or empty, headache, irritability, lack of appetite, loss of interest or pleasure, nervousness, painful or difficult urination, pounding in the ears, ringing in the ears, slow or fast heartbeat, stomach pain, tingling of the hands or feet, trouble concentrating, trouble sleeping, unusual tiredness or weakness, unusual weight gain or loss, changes in behavior, thoughts of killing oneself, seizures, hyperparathyroidism, prolactin increased, polycythemia, increased hematocrit, thrombocytopenia, anemia, diabetes mellitus, fluid retention, hyperlipidemia, hypertriglyceridemia, increased blood glucose, Korsakoff’s psychosis nonalcoholic, male orgasmic disorder, restlessness, sleep disorders, cerebrovascular insufficiency, reversible ischemic neurological deficiency, transient ischemic attacks, and amnesia. Marked affective and psychotic symptoms have also long been documented, symptoms which would often disqualify Service Members from military service.51
Military Psychiatric Retention and Potential Medical Evacuation Concerns
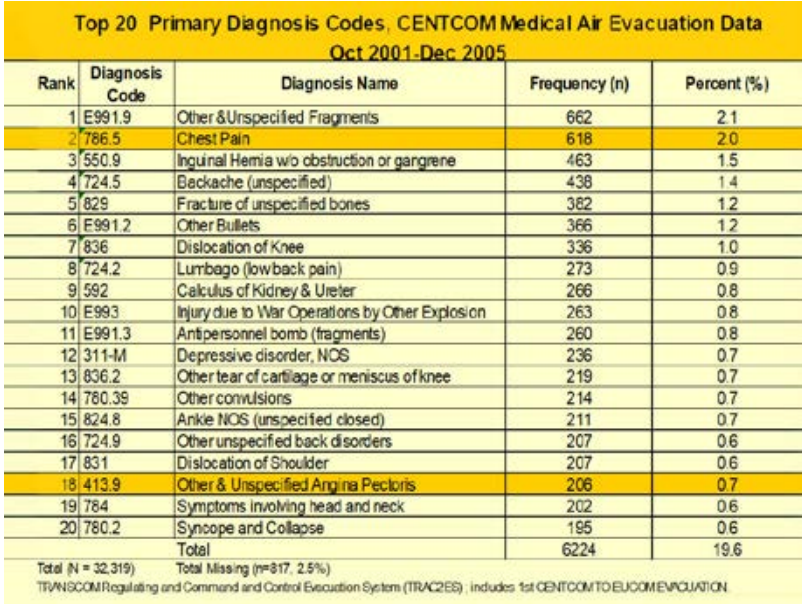
It is of interest here to note that one of the most frequent debilitating disorders in terms of medical evacuation, especially in hostile deployment theaters such as the Middle East, involve cardiac events – the very same events which can be precipitated or exacerbated by testosterone use. One of the major contributors to health care burden in the U.S. Armed Forces during Operation Iraqi Freedom was that of cardiovascular diseases,60 accounting in 2005 alone for a total of 1,369,581 person years of disability at an annual rate of 5.8 percent. CENTCOM medical air evacuation data from 2001 to 2005 show a stunning number of evacuations for both cardiovascular diseases, as well as depressive disorders, both of which may be associated with testosterone use.
Recent reports have indicated even higher levels of risk, with the danger levels for males taking cross sex hormones increasing by as much as 93%. According to a Danish study published in August in the European Journal of Endocrinology1 both sexually confused men and women developed a “significantly increased risk” of developing high blood pressure and high cholesterol and were more likely to have heart attacks and strokes. Males on opposite sex hormones were 93% more likely to develop a heart issue than men not taking hormones and 73% more likely than biological women. Biological women taking testosterone were found to be 63% more likely to have heart disease than women not taking hormone treatments and have over twice the risk of developing a heart condition as were biological men.
With data such as these, the risks of androgen use on active military service, especially in areas with less-than-optimal Echelon IV and V Level care, cannot be avoided. Echelon IV care includes full medical and surgical care, along with further definitive therapy for those patients in recovery phases. Echelon V provides full convalescent, restorative, and rehabilitative care, treatment often needed by cardiac patients; neither Echelon IV nor V care can be provided in deployed areas.
Stamps et al. (2006)
Concerns with Estrogen Abuse
Estradiol is the most potent and ubiquitous member of a class of steroid hormones called estrogens. Fetuses and newborns are exposed to estradiol derived from their mother, their own gonads, and synthesized locally in their brains. Receptors for estradiol are nuclear transcription factors that regulate gene expression, but also have actions at the membrane, including activation of signal transduction pathways. The developing brain expresses high levels of receptors for estradiol. The actions of estradiol on developing brain are generally permanent and range from establishment of sex differences to pervasive trophic and neuroprotective effects. The specific mechanisms of estradiol action permanently impacting the brain are regionally specific and often involve neuronal/ glial crosstalk. The introduction of endocrine disrupting compounds into the environment that mimic or alter the actions of estradiol has generated considerable concern, and the developing brain is a particularly sensitive target.42
Animal models indicate that experimentally induced alterations in the levels of steroid hormones, particularly estradiol, in the brain cause significant behavioral changes observable within minutes, leading some researchers to conclude that steroid hormones actually have the capacity to function directly as neurotransmitters in the central nervous system. In the nervous system, estradiol plays an important role in a wide range of neurological functions. To this end, estradiol is involved in fine motor control, learning, memory, sensitivity to pain, motor coordination, and protecting the brain against stroke damage and Alzheimer’s disease. Verbal memory, spatial ability, and fine motor skills are all influenced by estrogens. Estrogens are also involved in the strategies used to solve spatial or navigational puzzles which, as a result of their differences in estrogen levels, differ between males and females.53 Declines in estrogen have been associated with a number of changes in the brain, including cognitive changes, and effects on both sleep and moods. Furthermore, estrogen interactions have been indicated in a number of neuropsychiatric disorders, including Alzheimer’s disease, schizophrenia, and depression.56
Note also that toxic substances, such as male hormones introduced into a female body, will therefore inevitably be at biological “war” with the biologically authentic commands of the appropriate cells and chromosomes, resulting in eventual damage and dysfunction to the body that has been mistreated. This is also settled science and cannot be argued or disputed. One of the easiest ways for laymen to understand this fully is to look at some of the abnormalities produced in East Germany before the fall of the GDR (the German Democratic Republic) with their sex hormone experiments. Androgen abuse originated in the 1950’s, a product of the Cold War, whereby communist Eastern European countries could develop national programs to achieve short-term propaganda victories over the West in Olympic and international sports.26 The senior author was recently able to review some of these files personally while on a research trip to East Germany in March of 2019. The destruction of lives stemming from those taking these drugs, many of which are the same as are given to patients who want “to change their sex,” was so egregious, that they were even included in a movie about East Germany and shown widely throughout Germany as well as English speaking countries – The Weissensee Saga.72
Deployment Concerns
In order to be an effective Soldier, Sailer, or Airman, the Service Member must be available and fit for deployment throughout the world, whenever and wherever needed. Indeed, such military readiness is a prerequisite to military service.2 Therefore, deployment limitations demonstrated by sexually confused individuals may present a mission-jeopardizing problem for Commands.
Since ALL sexually confused individuals are mentally ill by their own definition, and as many as 80 percent display a large number of co-morbid disorders, deployment Commands must anticipate higher risks of psychiatric emergencies, disorders, and medical burdens upon medical treatment facility (MTF) staff with this group of Soldiers. The risk factor must also logically lead to increased risk factors for wartime theater evacuation due to these issues, as well as potential medication complications. Many of these guidelines were previously reviewed in the directives issued from United States European Command (USEUCOM).19
The use of psychoactive medications poses additional risks in the deployment environment, such as risk for heat injury, serotonin syndrome, lapses in judgment and alertness, etc. These medications are commonly used to treat depression, insomnia, drowsiness, concentration and alertness problems, mood disorders, anxiety, chronic pain, migraine headaches, seizures, etc.
Some of the conditions related to endocrine disorders have previously been summarized in Table B-5 and demonstrate the difficulty in managing some of these circumstances under conditions of deployment. The psychiatric disorders list is extensive and will not be repeated here, but almost any of these disorders could be manifested by sexually confused individuals with these co-morbid disorders. These sexual disorders are mentioned in Table B-18 and the risks of suicide, psychiatric disorders, and psychiatric burden are clearly identified. (See Table B-18 on page 19.)
Eventual Anticipated Military Burdens
It is therefore abundantly clear that despite the naïve statements or even willful rejection of scientific evidence by influential but naïve figures such as Jocelyn Elders, David Satcher, Ashton Carter and others that sexually confused individuals may be “perfectly fit” for military service, the opposite is quite true, and substantial military burdens are expected from the attempted integration of such individuals into the Armed Forces. Unfortunately, this mirrors very closely the previous disaster with the “McNamara’s 100,000” project in that repeated warnings from mental health professionals and experienced military personnel who well understood the issues of both strenuous military service and mental handicaps, these being so callously and cavalierly dismissed for political gain. At least 80 percent of sexually disturbed individuals will demonstrate co-morbid mental disorders and as many as 40 percent may demonstrate suicidal ideation or attempts, greatly increasing the demands upon military health care providers. Among the psychiatric disorders manifested, the very fact that such individuals reject reality in terms of rejecting basic biology, are excessively narcissistic and may also frequently defy authority as well as display marked difficulties with social mores that are manifested by most of society will inevitably create problems in many military units. This will also negatively impact military members at large and in addition, can be expected to increase friction within the service and probably among the ranks, with more “Bradley Manning” and “Jamie Henry” types of incidents are likely to occur. Furthermore, the tendency of this group of individuals to demonstrate narcissism, to reject the social mores of “normals” and to blame everyone else for “bias,” etc., rather than facing issues stemming from their own adjustment struggles, will not be helpful in this regard. The substantial medical and neurophysiological burden increased by the use of “cross sex” drugs will also tend to substantially increase medical needs and care factors for this cohort and may eventually result in many of them being unfit for service or deployment. The combined factors of pre-existing co-morbid psychiatric disorders, as well as medications use, will also undoubtedly result in many such individuals being increasingly vulnerable to stress-related disorders encountered in the military, such as PTSD, and other disorders of depression and psychiatric debility. Once separated from active duty due to their disabilities, most of this cohort will presumably qualify for ongoing care and benefits from the Veteran’s Administration, also increasing the medical and financial burdens of those services.69 In accordance with the medical benefits package, VA provides care and treatment to Veterans that is compatible with generally accepted standards of medical practice and determined by appropriate health care professionals to promote, preserve, or restore the health of the individual69 (AUTHORITY: 38 U.S.C. § 7301(b); 38 C.F.R. § 17.38). Of course, such policies will inevitably increase the burden of care on the VHA and may even be postulated to encourage some of this cohort to join the service with the anticipation and goal of eventually receiving lifelong care, ensuring that the VHA is now their permanent “insurance policy,” consistent with the statements of Kenneth Zucker.73 In addition, hundreds of “detransitioners” are now coming forward35 and it is guaranteed that a number of sexually confused individuals will eventually decide to “detransition,” either while in active service or after transferring upon service separation to the VA. Jorgenson,35 in particular, outlines the long-term iatrogenic damages to such patients, the burden of care also inevitably falling to either the Armed Forces or the VA, much as the long term care for McNamara’s 100,000 eventually cost the United State millions of dollars.29
All of this must also be considered in terms of the ability of the military to provide such care; treatment being typically limited at best, even in Echelon IV and V areas of care, and certainly not in the majority of Command or deployed theaters. Because of the virtually certain increased substantial strains upon the military health care system as well as increased separation and morbidity rates, the risks of service must be very carefully considered and may eventually have significant implications for our conservation of the fighting forces. Let’s not repeat the “McNamara’s 100,000” catastrophe, especially when we have been so strongly advised in advance.
References
- Anderson, K. Heart disease risk skyrockets in trans people taking hormones, study finds. Daily Caller News Foundation. 6 October 2023.
- Army Regulation 40-501 Active Duty Enlisted Administrative Separations, Headquarters, Department of the Army, Washington, D.C, Army Regulation 636 – 200 Standards of Medical Fitness. 2007, Headquarters, Department of the Army, Washington, D.C.
- Austin, A., Craig, S. L., D’Souza, S., and McInroy, L. B. Suicidality among transgender youth: elucidating the role of interpersonal risk factors. Journal of Interpersonal Violence. 2022, 37 (5-6): NP2696-NP2718, 2022.
- Bagatell C. J, Heiman J. R, Matsumoto A. M, Rivier J. E, and Bremner W. J. Metabolic and behavioral effects of high-dose, exogenous testosterone in healthy men. Journal of Clinical Endocrinol Metabolism. 1994, 79: 561-567.
- Barnes, H. (2023). Time to think: the inside story of the collapse of Tavistock’s gender service for children. Swift Press. 2023, Great Britain.
- Biologydictionary.net Editors. “How Many Cells Are in the Human Body?” Biology Dictionary, 2021. Biologydictionary.net.
- Birdsong, D. Second Language Acquisition and the Critical Period Hypothesis. Routledge. 1999, p. 74. ISBN 978-1-135-67489-2.
- Carter, A. Directive-type Memorandum (DTM) 16-005, Military Service of Transgender Service Members (PDF). Secretary of Defense, Department of Defense. Archived (PDF) from the original on November 5, 2017. Retrieved October 31, 2017.
- Chen, D., Strang, J. F., Kolbuck, V.D., Rosenthal, S. M., Wallen, K., Waber, D. P., Steinberg, et al. Consensus Parameter: Research Methodologies to Evaluate Neurodevelopmental Effects of Pubertal Suppression in Transgender Youth. Transgender Health, 2020, 5, (4).
- Clark, L. Department of Defense (DoD) Quarterly Suicide Report (QSR). Defense Suicide Prevention Office (DSPO.) 2022, United States Department of Defense.
- Cone, C., and Oliverson, T. Texas House Bill 1686, Public Health Committee Testimony. 2023. 1:55:25/8:44:32.
- Christopher, R. and Hopewell, C. A. Psychiatric correlates of combat trauma in military personnel: PTDS and TBI TESI statistical analysis. Operation Iraqi Freedom and Operation Enduring Freedom. Psychological, Clinical, and Forensic Assessment. 2007, Reno, Nevada: ISBN 158028-16-4.
- Curtiss, S. (2014). Genie: A Psycholinguistic Study of a Modern-Day Wild Child. Elsevier Science. 10 May 2014, p. 207.
- Daubert V. Merrell Dow Pharmaceuticals Inc., 509 U.S. 579, 1993.
- De Sanctis V., Soliman A. T., Di Maio S., Soliman N., and Elsedfy H. Long-term effects and significant adverse drug reactions (ADRs) associated with the use of gonadotropin-releasing hormone analogs (GnRHa) for central precocious puberty: A brief review of literature. Acta Biomed. 2019, 3: 345–359.
- Diagnostic and Statistical Manual of Mental Disorders V Edition TR. American Psychiatric Publishing. 2022, Washington, D.C.; London, England.
- Doombos, C. Navy SEAL training commander speaks out after scathing report on ‘shattering’ candidate death. New York Post. June 4, 2023.
- Elders, J., Satcher, D Former Surgeons General Debunk Pentagon Assertions about Medical Fitness of Transgender Troops (Press release). The Palm Center. 2018, Archived from the original on March 30, 2018. Retrieved March 29, 2018.
- United States European Command (USEUCOM) Theater Medical Entry Requirements. July 3, 2019.
- de Vries A. L, Cohen-Kettenis P. T. Clinical management of gender dysphoria in children and adolescents: the Dutch approach. Journal of Homosexuality. 2012, 59 (3): 301–320.
- Dhejne, C., Lichtenstien, P., Boman, M., Johansson, A. L. V., Langstrom, N., and Landen, M. Long-term follow-up of transsexual persons undergoing sex reassignment surgery: cohort study in Sweden. PLOS ONE. 2011, 6, (2).
- Dixen, J., M., Maddever, H., Van Maasden, J., et al. Psychosocial characteristics of applicants evaluated for surgical gender reassignment. Archives of Sexual Behavior. 1984, 13, (3): 269-277.
- Erlangsen, A., Jacobsen, A. L., and Ranning, A., et al. Transgender Identity and Suicide Attempts and Mortality in Denmark. JAMA 2023, 329 (24): 2145-2153.
- Ettner, R., Monstrey, S., and Eyler, A. E. (Eds). Principles of Transgender Medicine and Surgery. Haworth Press. 2007, New York.
- The Evolution of the Diagnosis of Gender Dysphoria Prevalence, co-occurring psychiatric diagnoses and mortality from suicide. Swedish National Board of Social Services, Socialstyrelsen. February 2020, Article number 2020-2-6600.
- Franke W. W, and Berendonk, B. Hormonal doping and androgenization of athletes: a secret program of the German Democratic Republic government. Clinical Chemistry. 1997, 43: 1262-1279.
- Galani, A., Kitsiou-Tzeli, S., Sofokleous, C., Kanavakis, E., and Kalini-Mavrou, A. Androgen insensitivity syndrome: clinical features and molecular defects. Hormones. 2008, 7 (3): 217–229.
- Goodman and Gilman’s The pharmacological basis of therapeutics. J. G. Hardman and L. E. Limbird (eds). McGraw Hill. 2002, New York.
- Gregory, H. McNamara’s Folly: The Use of Low-IQ Troops in the Vietnam War. Infinity Publishing. 2015, West Conshohocken, PA.
- Haas, A. P., Rodgers, P. L., and Herman, J. Suicide Attempts Among Transgender and Gender Non-Conforming Adults: Findings of the National Transgender Discrimination Survey. Williams Institute, UCLA School of Law. January 2014.
- Hopewell, C. A. Neuropsychology in the U. S. Army Europe. Medical Bulletin of the U.S. Army, Europe. 1983, 39, (10): 9-15.
- Hopewell, C. A, and Ozburn, M. S. Predicting graduation and rehabilitation success among low back pain patients enrolled in basic combat training. Medical Bulletin of the U.S. Army, Europe. 1979, 36 (3): 11-16.
- Hougha, D., Bellinghama, M., Haraldsenb, I. T., McLaughlinc, M., Robinsona, J. E., Solbakk, A. K., and Evans, N. P. A reduction in long-term spatial memory persists after discontinuation of peripubertal GnRH agonist treatment in sheep Psychoneuroendocrinology. 2017, 77: 1-8.
- Jewett, C. Kaiser Health News. February 2, 2017.
- Jorgensen, S. C. Iatrogenic Harm. Gender Medicine, Journal of Sex & Marital Therapy. 2023, June 19: 1-6.
- Kean, S. The Soviet Era’s Deadliest Scientist Is Regaining Popularity in Russia. The Atlantic. December 19, 2017.
- Klimas, J. No medically valid reason to exclude transgender troops, AMA chides Mattis. Politico. Archived from the original on April 5, 2018. Retrieved April 5, 2018.
- Luk, J. W, Goldstein, R. B., Yu, J, Haynie, D. L., and Gilman, S. E. Sexual Minority Status and Age of Onset of Adolescent Suicide Ideation and Behavior. Pediatrics. 2021, 148 (4): 1-10.
- Manning, B. The years since I was jailed for releasing the ‘war diaries’ have been a rollercoaster. The Guardian. Retrieved May 28, 2015.
- Mathy, R. M. Transgender Identity and Suicidality in a Nonclinical Sample: Sexual Orientation, Psychiatric History, and Compulsive Behaviors. Journal of Psychology & Human Sexuality. 2003, 14, (4): 47-65.
- Mayer, L.S. and McHugh, P. R. (Sexuality and Gender. The New Atlantis. 2016).
- McCarthy, M. Estradiol and the developing brain. Physiological Reviews. 2008, 88 (1): 91-134.
- Meybodi, A., M., Hajebi, A., and Jolfaei, A., G. The frequency of personality disorder in patients with gender identity disorder. Medical Journal if the Islamic Republic of Iran. 2014, 28 (90).
- Mihai, A. Mind Blowing Cases of Children Raised by Animals. ZME Science. 2014, 1 December.
- Morgan, R. 1st openly trans Army officer arrested for trying to pass secrets to Russia. American Military News, September 29, 2022.
- Moore, B. A., Hopewell, C. A., and Grossman, D. Violence and the warrior, In Living and Surviving In Harm’s Way: A Psychological Treatment Handbook for Pre- and Post-Deployment. 2009, S. M. Freeman B. A. Moore, and A. Freeman, (Eds.) Routledge: New York.
- Oliverson, T. Texas State House of Representative Public Health Committee Testimony, March 27, 2023. 1:55:25/8:44:32.
- Oury, J. P. The Lysenko affair: a comeback for the Fake News that led to millions of deaths? European Scientist. 2019.
- Pinsky, L., Erickson, R. P., and Schimke, R. N. Genetic Disorders of Human Sexual Development. Oxford Monographs on Medical Genetics. 1999, 38 (1).
- Pope, H. G., and Katz, D. L. Affective and psychotic symptoms associated with anabolic steroid use. American Journal of Psychiatry. 1988, 145: 487-490.
- Rametti, G., Carrillo, B., Gómez-Gil, E., Junque, C. Zubiarre-Elorza, L., Segovia, S., Gomez, Á., and Guillamon, A. The microstructure of white matter in male to female transsexuals before cross-sex hormonal treatment. A DTI study. Journal of Psychiatric Research. 2011, 45, (7): 949-954.
- Risk of pseudotumor cerebri added to labeling for gonadotropin-releasing hormone agonists.” publications.aap.org. 1 July 2022 eISSN 1556-3332. Retrieved 18 August 2022.
- Robertson, S. Estrodiol and the brain. News – Medical.Net. 2023.
- Roselli C. F. Brain aromatase: roles in reproduction and neuroprotection. Journal of Steroid Biochemistry and Molecular Biology. 2007, 106: 143-150.
- Rosenthal S. M. Transgender youth: current concepts. Annals of Pediatric Endocrinology & Metabolism. December 2016, 21 (4): 185-192.
- Russell, J. K., Jones, C. K., and Newhouse, P. A. The Role of Estrogen in Brain and Cognitive Aging. Neurotherapeutics. July 2019, 16 (3): 649-665.
- Sanchez, D. Former Army psychologist raises alarm on transgender soldiers. Epoch Times. July 5, 2023 – 11, 44.
- Schilling, C. Fort Hood postmortem: Crisis in psychological testing. World Net Daily. April 13, 2014, at 7:30 pm.
- Singal, J., How the Fight Over Transgender Kids Got a Leading Sex Researcher Fired. New York Magazine. 2016.
- Stamps, K., Jordan, N., Morrison, S., Marin, R., and Tobler, S. Cardiac Events in the Central Command Area of Operations (CENTCOM AOR). Force Health Protection Conference. August 9, 2006, Albuquerque, New Mexico.
- Strom, D. Army exempts trans service members from physical fitness standards. Hot Air. 3:31 PM on July 6, 2023.
- Swerdloff, R. S., and Heber, D. Superactive gonadotropin – releasing hormone agonists. Annual Review of Medicine. 1983, 34: 491-500.
- Terhune, C., Respaut, R., and Conlin, M. As children line up at gender clinics, families confront many unknowns. Reuters. October 6, 2022, Retrieved October 10, 2022.
- Transgender Service Member Policy Implementation Fact Sheet (PDF). Department of Defense. Archived (PDF) from the original on December 5, 2017. Retrieved November 28, 2017.
- Transgender Trend: Keira Bell: The high court hands down a historic judgment to protect vulnerable children. December 1, 2020.
- United States European Command (USEUCOM) Theater Medical Entry Requirements. United States European Command Instruction. ECI 4202.01. July 3, 2019. A-4 Enclosure A. UNCLASSIFIED.
- Uzych, L. Anabolic-androgenic steroids and psychiatric-related effects: a review. Canadian Journal of Psychiatry. 1992, 37: 23-28.
- Vrangalova, Z. There’s Growing Evidence For A Link Between Gender Dysphoria And Autism Spectrum Disorders. Forbes. November 15, 2017.
- VHA Directive 1341(3) AUTHORITY: 38 U.S.C. § 7301(b); 38 C.F.R. § 17.38.
- Warrier, V., Greenberg, D. M., Weir, E., Buckingham, C., Smith, P., Lai, M. et al. Elevated rates of autism, other neurodevelopmental and psychiatric diagnoses, and autistic traits in transgender and gender-diverse individuals. Nat Commun. Aug 7, 2020, 11 (1): 3959.
- Yanovski, J. A., Rose, S. R., Municchi, G., M. D., Pescovitz, O. H., Hill, S. C., Cassorla, F. G., and Cutler, Jr., G. B. Treatment with a Luteinizing Hormone – Releasing Hormone Agonist in Adolescents with Short Stature. New England Journal of Medicine, March 6, 2003, 348: 908-917.
- Weissensee Das Erste. 2010, Berlin, Deutschland.
- Zucker, K. Personal communication, September 23, 2020.
ABOUT THE AUTHORS

Dr. Alan Hopewell holds four degrees and four foreign language certifications, to include his BS, MS and PhD in Clinical Psychology and a second Master of Science Degree in Clinical Psychopharmacology.
He received his formal Clinical Neuropsychological training during his residency at the University of Texas Medical Branch in Galveston in the Division of Neurosurgery where he was the very first student of Harvey Levin, PhD, ABPP.
Dr. Hopewell was commissioned upon his graduation from the Texas A&M Corps of Cadets. He has served as Chief of Psychology Service at Landstuhl Army Regional Medical Center, where he founded the initial Traumatic Brain Injury Laboratory and at Brooke Army Medical Center, among others. He was the first Army Officer Prescribing Psychologist to serve and to practice in a Combat Theater, where he was awarded the Bronze Star Medal for meritorious service during Operation Iraqi Freedom. He was subsequently awarded a Meritorious Service Medal as he was a primary target during the Ft. Hood Jihadist Terrorist attack by his colleague, Nidal Hasan.
A former president of the Texas Psychological Association, he was also Awarded the Texas Psychological Association Award as the Outstanding Clinical Neuropsychologist in Texas.
He is currently Assistant Professor of Psychiatry and Behavioral Medicine, University of North Texas Health Science Center and maintains his practice in Fort Worth. He has been married for 48 years, has two sons, and is just now expecting his first grandson. His father, LTC Clifford Hopewell, a B-17 navigator prisoner of war, was the stenographer for the infamous Stalag Luft III prison camp in Germany (The Great Escape).
Based upon his combat service and as a prescribing psychologist, he was awarded one of the highest honors of the American Psychological Association, being elected a Fellow of the APA. He is currently an Assistant Professor of Psychiatry and Behavioral Medicine at the University of North Texas Health Science Center.

Dr. Robert Klein is a former Army psychologist with a PhD in clinical psychology. He is currently in private practice and conducts research involving active-duty military personnel and Veterans. His research publications and professional presentations focus on statistics and neuropsychology. Prior to becoming a psychologist, he was an US Army Airborne Ranger and qualified Infantryman. During his infantry time, he served on the Korean DMZ. Dr. Klein is also an OIF II Veteran.
Combat Stress Magazine
Combat Stress magazine is written with our military Service Members, Veterans, first responders, and their families in mind. We want all of our members and guests to find contentment in their lives by learning about stress management and finding what works best for each of them. Stress is unavoidable and comes in many shapes and sizes. It can even be considered a part of who we are. Being in a state of peaceful happiness may seem like a lofty goal but harnessing your stress in a positive way makes it obtainable. Serving in the military or being a police officer, firefighter or paramedic brings unique challenges and some extraordinarily bad days. The American Institute of Stress is dedicated to helping you, our Heroes and their families, cope with and heal your mind and body from the stress associated with your careers and sacrifices.